Morgenstern, J. The MINT trial: liberal or restrictive transfusion in MI, First10EM, December 25, 2023. Available at:
https://doi.org/10.51684/FIRS.133356
Throughout the length of my career, we have consistently heard that less is more when it comes to blood transfusions (outside of the critically ill requiring massive transfusion, where the message, correct or not, has been the exact opposite). This has been aided by the rise of intravenous iron, giving us an alternative effective option for patients with chronic or subacute anemia. However, there has always been some concern about translating this research into subgroups who may require more oxygen carrying capacity, such as those with acute coronary syndrome. That brings us to the Myocardial Ischemia and Transfusion (MINT) trial.
The paper
MINT: Carson JL, Brooks MM, Hébert PC, et al; MINT Investigators. Restrictive or Liberal Transfusion Strategy in Myocardial Infarction and Anemia. N Engl J Med. 2023 Nov 11. doi: 10.1056/NEJMoa2307983. Epub ahead of print. PMID: 37952133
The Methods
The MINT trial is an open-label, multi center RCT from 144 sites in the United States, Canada, France, Brazil, New Zealand, and Australia.
Patients
They enrolled adult patients with myocardial infarctions (both STEMI and NSTEMI) and anemia (hemoglobin less than 10 g/ deciliter or 100 g/L).
Intervention
“In the restrictive-strategy group, transfusion was permitted but not required when the hemoglobin level was less than 8 g per deciliter and was strongly recommended when the level was less than 7 g per deciliter or when anginal symptoms were not controlled with medications.”
Comparison
“In the liberal-strategy group, one unit of packed red cells was administered after randomization and red cells were transfused to maintain the hemoglobin level at or above 10 g per deciliter until the time of hospital discharge or 30 days.”
Outcome
The primary outcome was a composite of MI and death up to 30 days after randomization.
The Results
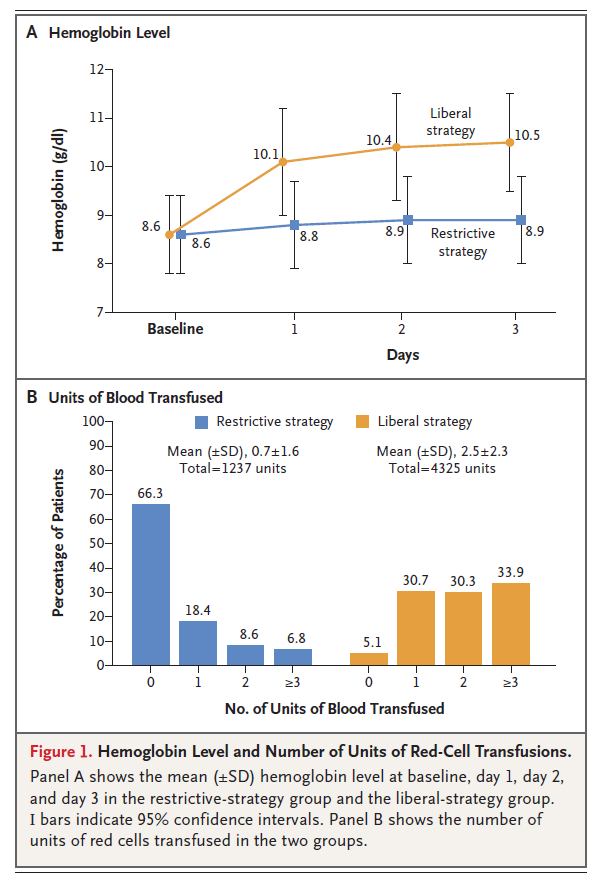
The MINT trial enrolled 3506 patients, and 3504 are included in the analysis. The mean age was 72 and 45% were women. The majority of patients had type 2 MIs (56%), with 42% having type 1. The mean hemoglobin at enrollment was 86 g/L.
There was a clear difference between the groups in terms of treatment given, and the difference seems large enough to be clinically significant. The mean hemoglobin rose by about 10 g/L in the liberal group and stayed the same in the restrictive group. However, significantly more of the liberal group had to have their protocol discontinued (14% vs 3%) for adverse events such as fluid overload.
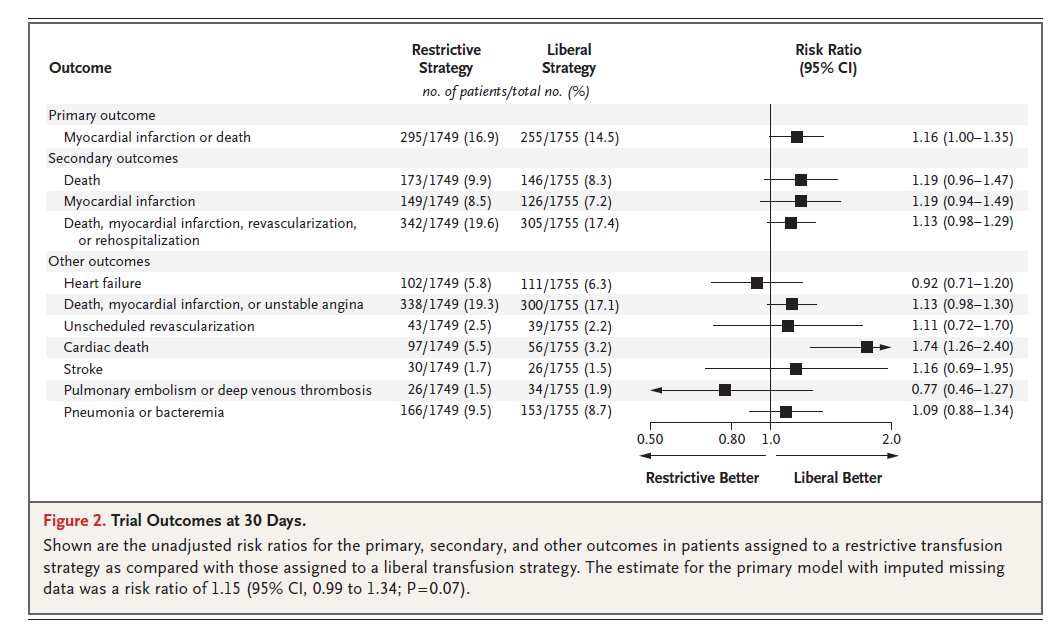
The primary composite outcome was not statistically different (16.9% in the restrictive group and 14.5% in the liberal group, RR 1.16, 95% CI 1.00 to 1.35).
Mortality was 9.9% in the restrictive group and 8.3% in the liberal group. MI was 8.5% in the restrictive group and 7.2% in the liberal group.

My thoughts
The MINT trial is going to bring out a lot of strong opinions from stats nerds. What does it mean when a 95% confidence interval touches but doesn’t cross 1? I think it is important that we recognize that trials are not a binary ‘positive’ or ‘negative’, and that there is always something to be learned by looking at point estimates. However, the folks that want to emphasize the point estimate and borderline statistical significance of this trial are likely to overlook 2 very important points. First, we use ridiculously lax statistical cutoffs in medicine, making false positive research much more likely than false negative. Second, and more important, when considering small differences in research trials it is essential to consider bias.
Statistically speaking, basically the entire range of the 95% confidence interval is better with the liberal strategy, so the math doesn’t seem all that complicated. However, that estimate needs to be adjusted for the many sources of bias. This is an unblinded trial. Parts of the protocol, such as treating when ‘angina is not controlled by medications’, are very subjective. They used a composite outcome, half of which (MI) is actually pretty subjective and not always clinically important. (A small rise and fall in troponin with no other clinical impact, especially in the context of an admission for another illness, is generally meaningless.) (O’Fee 2021)
Although myocardial infarction was adjudicated by blinded members of the research team, that doesn’t eliminate the significant bias that can occur in an unblinded trial. If clinicians are more nervous about patients with lower hemoblogins, they may order more ECGs and send more troponins, which will result in more positive results whether clinically significant or not.
The heterogeneity introduced by including both type 1 and type 2 MI seems like a mistake. This is especially true when a major cause of demand ischemia is anemia or acute bleeding. Oddly, in the subgroups there appears to be no difference in patients with type 2 MIs, but a statistical difference in type 1, which to me seems logically backwards. This might indicate bias, in that clinicians were allowed to break protocol, and they might be more likely to transfuse liberally in patients with demand ischemia, making the groups look more similar than they really are. It also bothers me that the manuscript does not contain more information about the causes of demand ischemia. It seems like it would make a huge difference whether demand was from sepsis or a GI bleed.
Ultimately this is a statistically negative trial with positive appearing point estimates. The only appropriate answer is “we don’t know”. We clearly need more research (and hopefully future research will do a better job separating out type 1 and type 2 MIs). There is no way that this trial should result in blanket treatment recommendations. Although there is a hint of benefit here, there are also known harms to transfusions, and we see that in this data, with significantly more patients experiencing volume overload and having to drop out of the trial in the liberal group. Although people hate the answer, we are going to have to apply clinical judgment until more research is completed. Given what we known about the harms of transfusion, and the propensity of clinical trials to underestimate harms, I think baseline practice should probably be closer to the restrictive group, but with lots of leeway for more liberal transfusion based on individual patient circumstances. (On the other hand, if you want to argue that liberal transfusion is usual care in MI right now, and that this data seems to support usual care, you won’t get a strong argument from me, as long as you allow restrictive transfusion based on clinical judgment and patient preference.)
Bottom line
The MINT trial is an important multicenter open label RCT comparing restrictive and liberal transfusion strategies in patients with MI, but it doesn’t give us definitive answers. Considering that most available data suggests benefit from restrictive transfusions, including in cardiac surgery, I think a baseline that is relatively restrictive makes sense, but clinicians will have to use their judgment to decide on the management of each individual patient.

Other FOAMed
Its been discussed a lot on Twitter, but I don’t think this trial has been discussed on any of by usual FOAMed sources yet (although I am writing this more than a month before it will be published, so hopefully that won’t be a lie when this comes out.)
Evidence based medicine is easy
Evidence based medicine resources
References
Carson JL, Brooks MM, Hébert PC, Goodman SG, Bertolet M, Glynn SA, Chaitman BR, Simon T, Lopes RD, Goldsweig AM, DeFilippis AP, Abbott JD, Potter BJ, Carrier FM, Rao SV, Cooper HA, Ghafghazi S, Fergusson DA, Kostis WJ, Noveck H, Kim S, Tessalee M, Ducrocq G, Gabriel Melo de Barros E Silva P, Triulzi DJ, Alsweiler C, Menegus MA, Neary JD, Uhl L, Strom JB, Fordyce CB, Ferrari E, Silvain J, Wood FO, Daneault B, Polonsky TS, Senaratne M, Puymirat E, Bouleti C, Lattuca B, White HD, Kelsey SF, Steg PG, Alexander JH; MINT Investigators. Restrictive or Liberal Transfusion Strategy in Myocardial Infarction and Anemia. N Engl J Med. 2023 Nov 11. doi: 10.1056/NEJMoa2307983. Epub ahead of print. PMID: 37952133
O’Fee K, Deych E, Ciani O, Brown DL. Assessment of Nonfatal Myocardial Infarction as a Surrogate for All-Cause and Cardiovascular Mortality in Treatment or Prevention of Coronary Artery Disease: A Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. 2021 Dec 1;181(12):1575-1587. doi: 10.1001/jamainternmed.2021.5726. PMID: 34694318