
Morgenstern, J. PE risk in severe exertional dyspnea, First10EM, June 26, 2023. Available at:
https://doi.org/10.51684/FIRS.130696
I think the conclusions of the paper are incredibly obvious, and therefore not practice changing, but I worry that a superficial read might lead to misinterpretation, and therefore the paper is probably worth covering. (This is the same research group that published the infamous PESIT study, and all the subsequent misinformation about PE risk in syncope, so it seems reasonable to be cautious). The question: what is the prevalence of PE in patients with acute onset, severe exertional dyspnea?
The paper
Prandoni P, Lensing AWA, Prins MH, et al. Prevalence of pulmonary embolism among patients with recent onset of dyspnea on exertion. A cross-sectional study. J Thromb Haemost. 2023 Jan;21(1):68-75. doi: 10.1016/j.jtha.2022.09.007. Epub 2022 Dec 22. PMID: 36695397
The Methods
This is a multicenter, prospective, cross-sectional study from 14 hospitals in Italy.
Patients
Adult patients (18-75 years) with less than a month of marked dyspnea during previously well-tolerated physical activities.
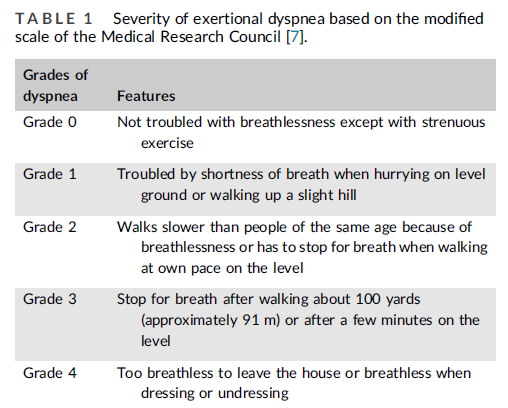
“Marked dyspnea” was defined as a severity of 3 or more on the modified Medical Research Council Dyspnea scale. This is defined as having to stop for breath after 100 yards or a few minutes of level walking. For comparison, a severity of 2 is “walks slower than people of the same age because of breathlessness or has to stop for breath when walking at own pace on the level”, and these patients were excluded from the trial.
Exclusions: Prior DVT or PE, therapeutic anticoagulation, contraindications to CTPA, or pregnancy.
Intervention/Comparison
All patients were worked up using a standard, validated PE algorithm, using the simplified Well’s score and an age adjusted D-Dimer.
Outcome
The primary outcome was the prevalence of PE.
The Results
Of 683 patients screened, 266 were excluded (mostly for not having severe enough dyspnea), leaving 417 patients in the overall study cohort. Of those, 213 had additional manifestations indicative of PE, and 94 (44%) of them ruled in for PE. Of the 204 that didn’t have additional PE manifestations, 40 (19.6%) ruled in for PE. Of those 204, 96 had apparent alternative explanations for the dyspnea (although the details are somewhat limited), and the rule in rate was still 14.6% in this subgroup.
Interestingly, they stopped the study based on a predefined end point, but then decided to run a second ‘validation study’ because the rule in rate was higher than they expected. They looked at an additional 61 patients with the same inclusion criteria, but this time excluding anyone with signs or symptoms of PE or clear alternative explanations, and in this cohort, the rule in rate was 30%.
My thoughts
I don’t find these results surprising at all, but perhaps the diagnosis of PE is taught differently around the world. The primary symptom of PE is dyspnea. People spend a lot of time talking about PE in the context of pleuritic chest pain, but the PE experts who taught me always emphasized that the primary symptom of PE is dyspnea. So if a young patient suddenly develops severe dyspnea on exertion, with no obvious cause, PE is near the top of the differential, whether or not they have classic VTE risk factors. If that is surprising to you, this study might be game changing, but for the rest of us, I think this just confirms usual practice.
The big risk from this study is that it gets over-applied, forgetting about the inclusion criteria. There are many reasons that patients develop mild exertional dyspnea, and working up every patient with a viral illness or seasonal allergies for PE could cause a lot of harm. However, in a patient with severe acute onset exertional dyspnea, there is no doubt that PE needs to be considered.
Based on past rule-in rates in Italy, we can anticipate that the rule in rate will be lower in other settings. However, considering the 20-30% rule in rate here, even if the rule in rate is half in Canada, these patients are still well above the test threshold, and warrant work up.
Bottom line
In what should be a surprise to no one, if a patient has severe dyspnea on exertion, PE is on the differential diagnosis. Just be careful not to extrapolate these findings to less severe or more vague symptoms.
References
Prandoni P, Lensing AWA, Prins MH, Ciammaichella M, Pirillo S, Pace F, Zalunardo B, Bottino F, Ageno W, Muiesan ML, Forlin M, Depietri L, Bova C, Costantini N, Caviglioli C, Migliaccio L, Noventa F, Levi M, Davidson BL, Palareti G; Pulmonary Embolism Dyspnea Italian Study (PEDIS) Investigators. Prevalence of pulmonary embolism among patients with recent onset of dyspnea on exertion. A cross-sectional study. J Thromb Haemost. 2023 Jan;21(1):68-75. doi: 10.1016/j.jtha.2022.09.007. Epub 2022 Dec 22. PMID: 36695397

3 thoughts on “PE risk in severe exertional dyspnea”
Maybe it’s an Italian thing?
Obvi…
I am glad that the article highlights the importance of considering PE in patients with severe exertional dyspnea. PE is a serious condition that can be fatal, so it is important to rule it out in these patients.