
Morgenstern, J. CRYOSTAT-2: Empiric cryoprecipitate in traumatic massive hemorrhage, First10EM, October 16, 2023. Available at:
https://doi.org/10.51684/FIRS.132356
In the massive hemorrhage deep dive, I mentioned that there were a number of large trials in the works that would further define practice. One of those trials – CRYOSTAT-2 – was just published, and adds important information about the role of empiric fibrinogen administration (in the form of cryoprecipitate) in trauma patients.
The paper
CRYOSTAT-2: Davenport R, Curry N, Fox EE, Thomas H, Lucas J, Evans A, Shanmugaranjan S, Sharma R, Deary A, Edwards A, Green L, Wade CE, Benger JR, Cotton BA, Stanworth SJ, Brohi K; CRYOSTAT-2 Principal Investigators. Early and Empirical High-Dose Cryoprecipitate for Hemorrhage After Traumatic Injury: The CRYOSTAT-2 Randomized Clinical Trial. JAMA. 2023 Oct 12. doi: 10.1001/jama.2023.21019.PMID: 37824155 NCT04704869
The Methods
CRYOSTAT-2 was a multicentre open-label RCT from 25 major trauma centers in the United Kingdom and 1 in the United States.
Patients
Adult patients (16 and older) with severe injury, systolic blood pressure less than 90 mmHg, and active hemorrhage requiring activation of the local massive hemorrhage protocol.
Exclusions: Being transferred from another hospital; injuries incompatible with life; more than 3 hours since the injury.
Common procedures
All patients were treated according to the local massive hemorrhage protocol, with an empiric 1:1:1 ratio of FFP, platelets, and packed red blood cells. Standard protocols also typically included 2 pools of cryoprecipitate (4-g fibrinogen equivalent) added to the second and subsequent packs. However, the exact approach was not standardized. For example, the US site used whole blood.
Intervention
3 units of empiric cryoprecipitate (approximately equivalent to 6 grams of fibrinogen) given as early as possible in the resuscitation.
Comparison
Usual care (there was no placebo).
Outcome
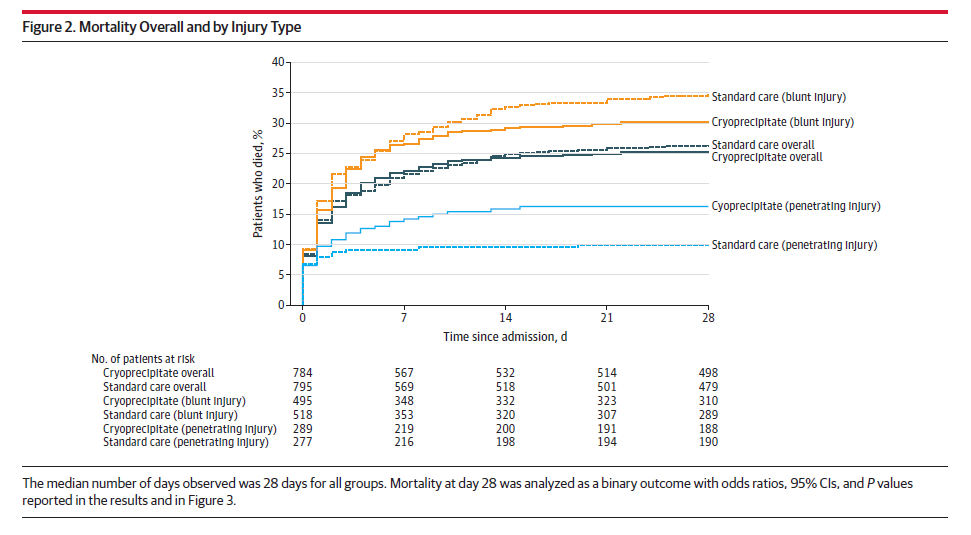
The primary outcome was all cause mortality at 28 days.
The Results
They enrolled 1604 patients, almost all of whom (1555) were enrolled in the UK. 1531 had outcome data available for the primary analysis. The median age was 39 years, and with a median injury severity score of 29. 26% had a severe head injury.
For the primary outcome, all cause mortality at 28 days was 25.3% with cryoprecipitate and 26.1% with standard care (OR 0.96; 95% CI 0.75-1.23; p=0.74). Mortality was also the same through all the other time frames observed from 6 hours to 12 months.
There were no differences in any of the secondary outcomes, including neurologic outcomes, transfusion requirements, hospital or ICU length of stay, or destination of discharge.
Thrombotic events were also the same (12.7% vs 12.9%).
My thoughts
CRYOSTAT-2 is a really important study, and should dampen enthusiasm for empiric fibrinogen therapy, but like all studies it is imperfect.
Unfortunately, I don’t think these results will generalize to most practice environments, because the massive hemorrhage protocol being used in the control group seems different than usual practice, at least in Canada. I am not sure how the choice to use a 1:1:1 over a 1:1:2 ratio for balanced transfusion impacts the effects of cryoprecipitate (although you could imagine that fibrinogen might be more important if you are less aggressive with FFP and platelets). However, my big concern is that all of these hospitals were already using empiric (rather than lab-guided) cryoprecipitate in the control group. Adding more cryoprecipitate to a protocol already using cryoprecipitate seems much less likely to provide benefit than adding empiric fibrinogen therapy to a protocol that isn’t giving any. For most hospitals around the world, it is the latter question we really need answered, and this study doesn’t provide us with an answer.
Protocol violations were very common. Of the 799 patients randomized to receive cryoprecipitate, only 434 actually receive the intervention, clearly biasing the intention to treat analysis towards the null hypothesis. This is in addition to the fact that cryoprecipitate was already being given at baseline in these protocols, so that by 24 hours 85% of the intervention group and 32% of the standard care group were given cryoprecipitate. However, the per-protocol analysis also showed no difference, which makes me less concerned about this specific source of bias.
Selection bias is a concern. They screened 9036 patients to find the 1604 enrolled, and although most exclusions were based on the inclusion criteria, 888 were because of lack of availability of the research team, and another 206 didn’t have the reason recorded.
I am not sure empiric therapy in massive hemorrhage makes a lot of sense (whether we are talking about fibrinogen, or the broader topic of empiric FFP and platelets in balanced ratios). Not all patients have coagulopathy at the outset of resuscitation, and giving blood products to patients who don’t need them is a mistake. Rapid testing, either with rapid bedside assessments of traditional measures like CBC, INR, calcium, and fibrinogen, or with viscoelastic testing, makes a lot more sense, as we can target appropriate blood products to patients who actually need them. If viscoelastic testing pans out, it will sort of render this study’s entire question moot.
Although we often lump all trauma patients together, trauma is a very heterogeneous presentation. One of my main concerns when looking at trauma studies is that outcomes in patients with head injuries (which are less likely to benefit from our massive hemorrhage protocols) will wash out outcomes in patients without head injuries. Only 26% of this population had a severe head injury, which makes me think this was a very good population to assess the utility of cryoprecipitate.
The required interventions and clinical trajectories for blunt and penetrating trauma are also quite different. I am very cautious about interpreting any subgroup analyses, but I imagine we will see follow-up research based on the appearance of worse outcomes in penetrating injury but possible better outcomes in blunt injury.
There are also some subgroups based one time, and although I have seen some people on social media talking about them, I would suggest ignoring them completely unless you are a researcher. With no placebo, the control group can’t be broken down by time. Therefore, these outcomes are just based on bad observational data, with a huge number of confounders. In the setting of significant trauma, time to an experimental intervention will be impacted by many things, such as the severity of injury, number of free IV lines, and the need for other interventions. All of these are much more likely to be the cause of mortality than slight variations in time to administration of cryoprecipitate.
There are a few previous trials of empiric fibrinogen in other settings, and the results are rather mixed. There is 1 RCT in postpartum hemorrhage that showed no benefit. (Wikkelsø 2015) There are a few other small studies in the context of aortic or cardiac surgery. One was stopped early because of harm (Rahe-Meyer 2016), but the others show a moderate decrease in blood loss or transfusion requirements. (Karlsson 2009; Rahe-Meyer 2009; Rahe-Meyer 2013) Overall, this is obviously an area of science with significant remaining uncertainty.
Bottom line
This is the first large RCT of empiric cryoprecipitate in trauma, and it is clearly negative. There are multiple sources of bias, and these results may not generalize to all practice settings. However, based on this study, I will continue my approach of rapid and frequent measurements of fibrinogen levels, with administration only when required (my threshold is 1.5 grams/L).
Other FOAMed
I haven’t seen this one covered anywhere yet, but I am sure it will be.
For now, you can read more about transfusion evidence than you ever wanted to here.
References
Davenport R, Curry N, Fox EE, Thomas H, Lucas J, Evans A, Shanmugaranjan S, Sharma R, Deary A, Edwards A, Green L, Wade CE, Benger JR, Cotton BA, Stanworth SJ, Brohi K; CRYOSTAT-2 Principal Investigators. Early and Empirical High-Dose Cryoprecipitate for Hemorrhage After Traumatic Injury: The CRYOSTAT-2 Randomized Clinical Trial. JAMA. 2023 Oct 12. doi: 10.1001/jama.2023.21019. Epub ahead of print. PMID: 37824155
Karlsson M, Ternström L, Hyllner M, Baghaei F, Flinck A, Skrtic S, Jeppsson A. Prophylactic fibrinogen infusion reduces bleeding after coronary artery bypass surgery. A prospective randomised pilot study. Thromb Haemost. 2009 Jul;102(1):137-44. doi: 10.1160/TH08-09-0587. PMID: 19572078
Rahe-Meyer N, Pichlmaier M, Haverich A, Solomon C, Winterhalter M, Piepenbrock S, Tanaka KA. Bleeding management with fibrinogen concentrate targeting a high-normal plasma fibrinogen level: a pilot study. Br J Anaesth. 2009 Jun;102(6):785-92. doi: 10.1093/bja/aep089. Epub 2009 May 2. PMID: 19411671
Rahe-Meyer N, Solomon C, Hanke A, Schmidt DS, Knoerzer D, Hochleitner G, Sørensen B, Hagl C, Pichlmaier M. Effects of fibrinogen concentrate as first-line therapy during major aortic replacement surgery: a randomized, placebo-controlled trial. Anesthesiology. 2013 Jan;118(1):40-50. doi: 10.1097/ALN.0b013e3182715d4d. Erratum in: Anesthesiology. 2013 May;118(5):1244. PMID: 23249928
Rahe-Meyer N, Levy JH, Mazer CD, Schramko A, Klein AA, Brat R, Okita Y, Ueda Y, Schmidt DS, Ranganath R, Gill R. Randomized evaluation of fibrinogen vs placebo in complex cardiovascular surgery (REPLACE): a double-blind phase III study of haemostatic therapy. Br J Anaesth. 2016 Jul;117(1):41-51. doi: 10.1093/bja/aew169. PMID: 27317703
Wikkelsø AJ, Edwards HM, Afshari A, Stensballe J, Langhoff-Roos J, Albrechtsen C, Ekelund K, Hanke G, Secher EL, Sharif HF, Pedersen LM, Troelstrup A, Lauenborg J, Mitchell AU, Fuhrmann L, Svare J, Madsen MG, Bødker B, Møller AM; FIB-PPH trial group. Pre-emptive treatment with fibrinogen concentrate for postpartum haemorrhage: randomized controlled trial. Br J Anaesth. 2015 Apr;114(4):623-33. doi: 10.1093/bja/aeu444. Epub 2015 Jan 13. PMID: 25586727




2 thoughts on “CRYOSTAT-2: Empiric cryoprecipitate in traumatic massive hemorrhage”