
Morgenstern, J. Delayed sequence intubation: An RCT, First10EM, September 25, 2023. Available at:
https://doi.org/10.51684/FIRS.131885
Introduced to the world by our friend Scott Weingart, delayed sequence intubation (DSI) is often summarized as procedural sedation for the procedure of preoxygenation. (Weingart 2011, Weingart 2015) It is a brilliant concept, makes a ton of sense on paper, and anecdotally has seemed to help a number of my patients. However, any long time reader will know how I feel about anecdote and theory. To date, the evidence has been virtually non-existent. This, as far as I know, is the first RCT of delayed sequence intubation.
The paper
Bandyopadhyay A, Kumar P, Jafra A, Thakur H, Yaddanapudi LN, Jain K. Peri-Intubation Hypoxia After Delayed Versus Rapid Sequence Intubation in Critically Injured Patients on Arrival to Trauma Triage: A Randomized Controlled Trial. Anesth Analg. 2023 May 1;136(5):913-919. doi: 10.1213/ANE.0000000000006171. Epub 2023 Apr 14. PMID: 37058727
The Methods
This is an open-label single center RCT.
Patients
Adult trauma patients with requirement for intubation.
Exclusions: Anticipated difficult airway, extensive burns, active vomiting, crash intubations, cardiac arrest. They also retrospectively excluded all patients with an unanticipated difficult airway, which makes no sense to me. (Discussed below.)
Intervention
Delayed sequence intubation. (IV ketamine 1.5 mg/kg in 0.5-mg/kg increments until dissociation was achieved (patient is calm but spontaneously breathing) followed by preoxygenation for 3 minutes followed by IV succinylcholine 1.5 mg/kg and endotracheal intubation.)
Comparison
Rapid sequence intubation. (Preoxygenation for 3 minutes followed by induction with intravenous ketamine 1.5 mg/kg and IV succinylcholine 1.5 mg/kg followed by endotracheal intubation.)
Shared procedures
Direct laryngoscopy was used in both groups. Intubation was done by second year anesthesia residents.
Outcome
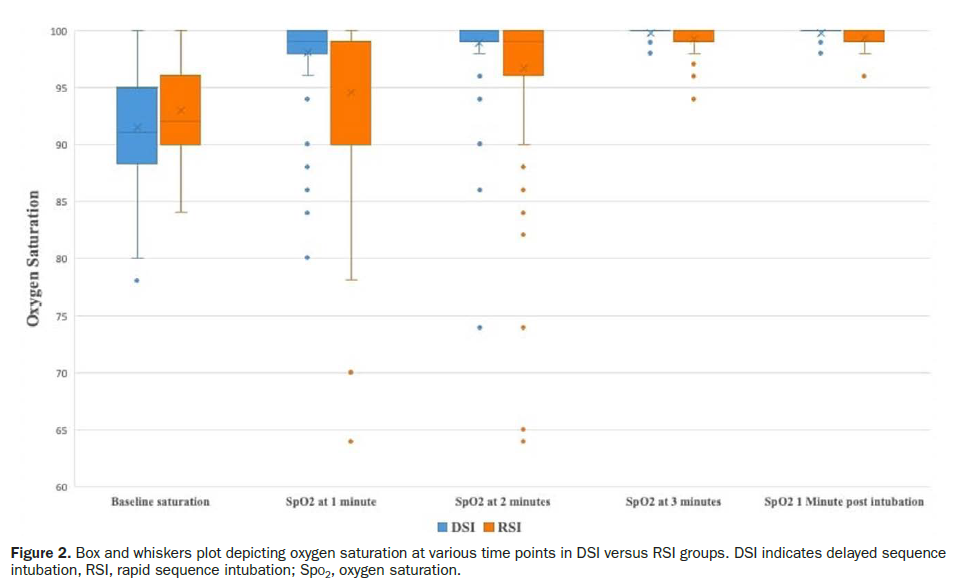
The primary outcome was peri-intubation hypoxia, defined as an oxygen saturation less than 93% anytime from preoxygenation to 1 minute post intubation.
The trial was preregistered, but unfortunately the manuscript doesn’t match the protocol perfectly.
The Results
The patients are as you would expect: young healthy males. 100% of patients in the RSI group were intubated because of mental status, whereas 5% of the DSI group had respiratory distress, which would bias the trial against DSI.
The primary outcome, peri-intubation hypoxia, was significantly lower in the DSI group (8% vs 25%, p<0.001)
First pass success was higher with DSI (83% vs 69%, p=0.02) Airway related adverse events were not statistically different, but favored DSI (9% vs 16%). There were no cardiac arrests or episodes of hypotension in this trial.
My thoughts
This is an important study, being the first RCT of DSI. Performing an RCT in sick trauma patients is no small feat, and the authors deserve credit for that. However, there are numerous issues with the study.
The fact that they retrospectively excluded all patients with an unanticipated difficult airway, which included not just a difficult intubation, but also difficulty with BVM and laryngoscopy, makes no sense to me, and has the potential to introduce significant bias. A known complication of ketamine is laryngospasm, so what if ketamine is the cause of all these unanticipated difficult airways? Conversely, proper pre-oxygenation should give you much more time to intubate, which will make even anatomically difficult airways seem easier. Excluding these patients makes no sense, because their outcomes seem to be intrinsically tied to the harms and benefits of DSI. There were only 36 patients excluded this way, but there was evidence of bias, in that twice as many patients were excluded in the RSI arm.
Their definition of peri-intubation hypoxia seems strange to me. First, I don’t care about an oxygen saturation of 92%. I am not sure why they didn’t use the more standard cut-off of less than 90%. More importantly, 1 minute might not be long enough to monitor after intubation, especially in shock states, where the peripheral oxygen saturation can lag the real saturation by many minutes. (I think their data might show this, as there are more hypoxic outliers at 2 minutes than at 1.)
There are some changes between the pre-registered protocol and the final publication. The original protocol says the primary outcome was going to be at 30 seconds, and the original protocol doesn’t say anything about retrospectively excluding difficult patients.
Selection bias is a real issue in this trial, in that there were over 1000 total intubations performed by this trauma service, but we are only looking at 200. Most exclusions were because the intubation occurred in the pre-hospital environment, or was performed by an emergency resident rather than the anesthesia resident.
They only preoxygenated with oxygen flows of 10 L/min, whereas I prefer flush rate. However, these intubations were performed by anesthesiologists using a Bain circuit, so we are comparing apples and mangos.
As the Driver bougie studies have taught us, generalization from airway studies can be very difficult. Skill of local operators can have dramatic impacts on the results. Personally, I think the first pass success in this trial is way too low in both groups (83% and 69%), especially considering they excluded anyone with a difficult airway. There are many reasons that first pass success can be low, but the use of direct laryngoscopy, and the fact that these were trainees intubating, means that I don’t believe I can extrapolate this data to my own practice.
The big issue with this paper, although also the most interesting aspect of this paper, is that it studies DSI in a population very different from that originally envisioned. DSI was originally described as a method of ensuring adequate preoxygenation in patients who are too agitated to tolerate preoxygenation. This study looks at DSI in all comers, which really should minimize the benefit of DSI, as there are a large number of trauma patients who tolerate normal preoxygenation without any difficulty. In that respect, this is a stronger argument in favour of DSI than even the baseline numbers suggest.
Bottom line
This is the first RCT of DSI, and the results favour DSI. However, it is a very low level of evidence, being an unblinded single center study, with multiple sources of bias. I think that it is reasonable to use DSI, but this in no way makes DSI the standard of care.
Other FOAMed
EMCrit: Delayed Sequence Intubation (DSI)
The RESUS Room Papers of August 2023
REBEL Cast Ep122 – Delayed vs Rapid Sequence Intubation in Agitated Trauma Patients
References
Bandyopadhyay A, Kumar P, Jafra A, Thakur H, Yaddanapudi LN, Jain K. Peri-Intubation Hypoxia After Delayed Versus Rapid Sequence Intubation in Critically Injured Patients on Arrival to Trauma Triage: A Randomized Controlled Trial. Anesth Analg. 2023 May 1;136(5):913-919. doi: 10.1213/ANE.0000000000006171. Epub 2023 Apr 14. PMID: 37058727
Weingart SD. Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. J Emerg Med. 2011 Jun;40(6):661-7. doi: 10.1016/j.jemermed.2010.02.014. Epub 2010 Apr 8. PMID: 20378297
Weingart SD, Trueger NS, Wong N, Scofi J, Singh N, Rudolph SS. Delayed sequence intubation: a prospective observational study. Ann Emerg Med. 2015 Apr;65(4):349-55. doi: 10.1016/j.annemergmed.2014.09.025. Epub 2014 Oct 23. PMID: 25447559



One thought on “Delayed sequence intubation: An RCT”