

In Korea where I (hi!) originally trained, because of fewer human resources (like radiologists), and an abundance of technological resources,(like CT and MRI) emergency physicians often are expected to read their own imaging. There are next-day overreads from Radiology, and patients are sometimes called back, but by and large, in-the-moment decisions are made by the EPs and their wet reads.
It felt like CT scans were everywhere there. And you know what? They’re everywhere here too. CT scans as performed by our emergency department about 4500 times a month, which boils down to a CT scan every 6 minutes! According to a recent report by the Ministry of Health of Ontario, a CT scan has an average turnaround time of about 2.5 hours. Does that make sense to you? Can you think of any other test that is ordered with that frequency, that takes that long to complete? It’s a significant delta. This is not Radiology’s fault, and this post, if anything, is meant to highlight the importance of working together with the invaluable expertise of Radiology as Emergency Physicians.
There are so many logistical factors that go into a completed CT scan, and one area we can take action on is the time spent waiting for a report. We pride ourselves in being the first and last line of defense and seeing “whatever comes through the door.” We do our own calculations for anion gaps and osmolar gaps and calcium corrections, we do our sutures, we intubate, we read high-stakes ECGs, and we even read our own brain CTs (!!!).
But as soon as the scanner goes a little bit south of the head, all of a sudden the pixels on the screen make no sense, and we can’t even. This needs to change. We need to start looking at our own scans, and when feasible, make some decisions.
Clinical Correlation Required
How many of you have looked at this comment in a report, and snorted “yeah, they always say that.” Clinical correlation, the age-old joke, is a cliché because it’s true.
This systematic review from 2020 looked at radiology reporting outcomes and how they are affected by clinical correlation. It was quite robust, comprising 21 studies with various imaging modalities going all the way back to 1963 for x-rays and included CT and MRI for studies up to 2019. The bottom line was that the accuracy, confidence and clinical relevance of the final report were significantly better when more clinical information was supplied to the image interpreter. There should be no surprise there. “Pain” as your requisition comment is, shall we say, a suboptimal amount of detail for your radiologist to give you the answers you seek.
No radiologist has spent as much time with the patient as you have, and thus you as the treating clinician are in the unique position of having the highest quantity and quality of clinical correlation to draw conclusions from. Let’s see if I can’t convince you that there are some good reasons you can and should be looking at your own CT images.
1. Obvious Findings = Obvious Disposition
When there are obvious pathological findings pointing to a clear diagnosis, call the appropriate consultants. You already do this with brain CTs, which by the way is a practice supported by pretty good evidence.
Nobody is asking you to measure the appendix wall thickness or stage a lymphoma.
Just have a look: is there a ton of free air on that CT for the patient who is febrile and peritonitic? Every surgical service has a habit of looking at their own CTs, and the surgical residents are more than capable of making a decision to at least come see the patient or not.
Some of you already do this with clear strokes and bleeds, intestinal obstructions and perforations. You are shortening time to disposition and thus time to treatment and length of ED stay, and inmproving the care of the patient.
When I asked why not disposition patients based off of wet reads, there were some interesting responses from our staff: everything from “because I value my license” to “we are already expected to do too much” all the way to “other services won’t believe us.”
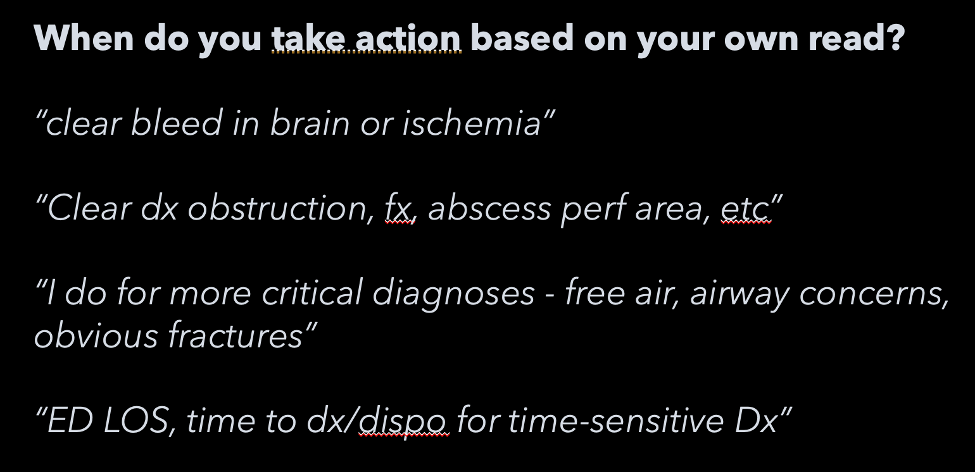
There are always going to be reasons not to do something new, something that has a degree of risk, or something that interrupts your usual workflow. But the good news is that, I assure you, terrible diagnoses on CT are easy diagnoses with obvious findings.
Remember – nobody is asking you to measure lymph node sizes or determine cancer stage here.
But if you see free air in the belly, you’d better be calling a surgeon to have a look.
2. Unclear findings must be made clear for better disposition
Rule #2 that I’m proposing is to call and discuss with the radiologist if the clinical does not in fact correlate. You already do this with x-rays and fractures.
I once saw a patient who was squeezed in between a dock and a boat, while in the water they were screaming in pain, but the preliminary report said there were no acute findings. I walked over and talked to the radiologist and after some hemming and hawing, we did eventually find that maybe there were signs of a very early psoas muscle bleed. That patient later required multiple ORs to control the hemorrhage, which Trauma was ready for due to the modified CT report.
Keep your friends close, and your radiologists closer.
A lot of you already look at your own images and call the radiologist when what you’re reading doesn’t match what you’re seeing. This is excellent.
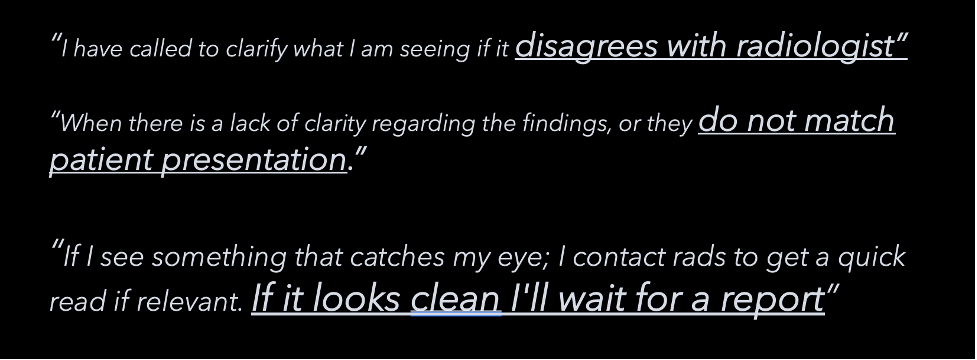
If you don’t see much up front, I think the right move is to wait for the report. I believe you’d all agree that the vast majority of risk involved with taking action based on our own reads would be if we were to declare CTs negative, and thus discharging patients home.
We don’t need to be sensitive, only specific – radiology can be sensitive for us.
3. Safer Handover: “Could you follow up on the CT report?”
Yet another reason to look at your own CTs is because it makes for a safer handover. We already know handover is a point of critical vulnerability in patient safety, and naturally we can and should do everything we can to minimize that risk. Patients are often handed over from one team to another for follow-up on imaging.
I propose that it should become standard practice for that handover to include a phrase like “I took a quick look myself and I don’t see any major bleed in the brain, or hemopneumothorax, or pneumoperitoneum, so could you please follow up on the formal report?”.
We look at everything else, like bloodwork, ECGs, urinanalysis, and x-rays before handing over. Why should CTs be any different?
4. You might have no choice
You may in fact have no choice but to look at your own CTs someday. It may not be today, it may not be tomorrow. But sooner rather than later, there may come a situation where either you don’t have a radiologist to read everything for you, or you may be part of a mass casualty incident where there are too many studies for radiology to process alone, or your institution may be hit by a cybersecurity incident. These seem to be becoming more ubiquitous by the day.
If this seems farfetched to you, have a look at this Google search. We practice and discuss resuscitative c-sections for our Royal College exam, but realistically, what’s more likely to happen?
Countries with less radiology resources than ours have quite a bit research looking into emergency physician proficiency in interpreting CTs. Many of these studies support the cautious use of ED physicians’ CT interpretations for patient management. There is also evidence that shows the earlier you start looking at your CTs, the more your practice pattern is likely to change.
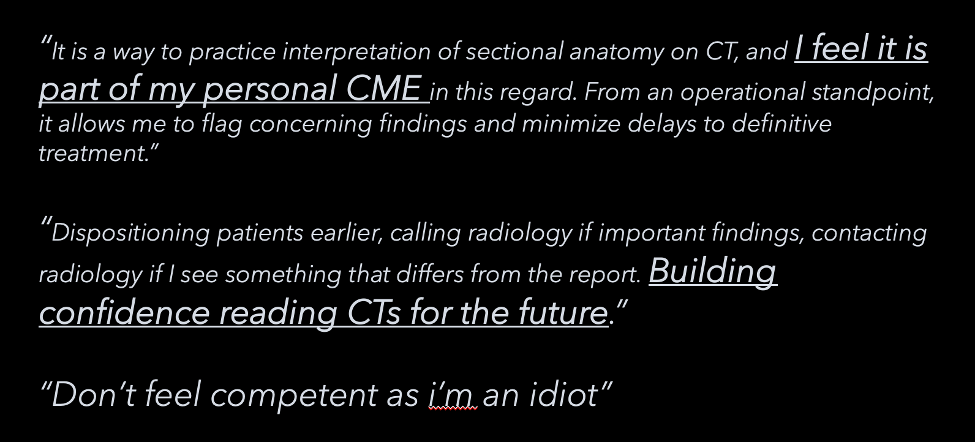
5. There are ways to get better
Even if you feel you’re terrible at reading CTs, it’s not as hard as you think, and there are easy ways to get better. It costs 60 dollars to get started with Radiopaedia’s fantastic online emergency radiology course (I have no financial interests to declare – only expenses ha). You can get better at it than you think.
A study from Japan looking at emergency physician CT interpretation accuracy for blunt trauma found, out of a total 1606 CTs, a miss-rate of 2.5%. And they estimated that only 7 patients’ (1.9%) clinical course was significantly altered.
If you’re going to sit there and tell me “those numbers are skewed because they look at their own CTs regularly” – well then you’ve just proven my point.
We accept way more than 1.9% of risk for a lot of things, on a daily basis.
In fact, the American College of Emergency Physician’s official stance is that emergency physcians are “expected to be competent in the interpretation of diagnostic imaging studies, including computed tomography scans.” Imaging, just like ECGs and bloodwork, is but part of a holistic clinical picture, and is the next logical step to include in our own overall assessment of our patients.
You don’t call cardiology for every ECG and you don’t call nephrology to interpret blood gases. An initial look at CT scans should be no different.
The Bottom Line
So here’s what I recommend.
- You don’t have to open every single CT.
- You don’t even have to do it regularly during your shift.
- Instead, I recommend starting with taking a look at the CT scans that are pending reports, exclusively in the last 2 hours of your shift.
- This will help you determine disposition for clear-cut cases with clear-cut findings on CT, or page radiology for clarification, and from a safety perspective, avoid handing over ticking time bombs.
