
As usual, a random smattering of articles. This group was presented as part of a live podcast recording at Sir Charles Gairdner Hospital in Perth, Australia, where I was honoured to be invited to be the WG Smith visiting lecturer. The guests helped select the papers, which means they are just as random as usual.
The TXA issue settled once and for all?
PATCH-Trauma Investigators and the ANZICS Clinical Trials Group; Gruen RL, Mitra B, et al. Prehospital Tranexamic Acid for Severe Trauma. N Engl J Med. 2023 Jun 14. doi: 10.1056/NEJMoa2215457. Epub ahead of print. PMID: 37314244
TXA might be the most intensively studied intervention in all of emergency medicine, so the fact that there are still major questions about its utility really says something. The PATCH-TRAUMA trial is a prehospital double-blind, placebo controlled RCT essentially replicating CRASH2 (with the same TXA doses and infusion) in a prehospital setting. Given the association between earlier administration and better outcomes (and later administration and death), if TXA works, you would expect it to work even better when given in the prehospital setting. This trial enrolled 1310 patients, with 1131 left in their final intention to treat analysis. The primary outcome was a favourable functional outcome at 6 months, and there was no benefit (53.7% vs 53.5%, RR 1.00, 95%CI 0.9-1.12, p=0.95). That sounds like a pretty damning CRASH2 replication, but it is complicated by the secondary outcome of mortality. Mortality was also not statistically different at 6 months, but the point estimate favours benefit, and there was a statistically significant benefit in 24 hour and 28 day mortality. That makes this trial difficult to interpret. It is an overall negative trial, but it is obviously much much smaller than CRASH 2, so probably not enough to overrule those results. There might be a mortality benefit that matches CRASH2. However, it also looks like we might just be shifting deaths to severe disability, which might actually be considered harm by our patients. There are significant sources of bias in this trial, including 35% of patients having protocol violations, significant loss to follow-up, and indication of significant selection bias. Given that every major TXA trial since CRASH2 has been negative, I remain very skeptical about TXA overall. I have always guessed that a replication of CRASH2 would be negative. That being said, despite technically being negative, this trial really doesn’t settle things.
Bottom line: This is a double blind, multicentre, prehospital trial of TXA for patients with severe trauma and predicted trauma induced coagulopathy. There was no difference in the primary outcome of 6 month survival with good functional status. However, these results are probably not enough to overrule the CRASH2 trial, and therefore I don’t think practice should (or will) change based on this trial.
Unconditional cash transfers reduce homelessness
Dwyer R, Palepu A, Williams C, Daly-Grafstein D, Zhao J. Unconditional cash transfers reduce homelessness. Proc Natl Acad Sci U S A. 2023 Sep 5;120(36):e2222103120. doi: 10.1073/pnas.2222103120. Epub 2023 Aug 29. PMID: 37643214
Although I think we all now recognize the fundamental importance of social determinants of health, I don’t think emergency medicine has found a way to adequately integrate this into our care. That is a shame, considering the huge amount of effort we put into things like tetanus shots or TXA therapy that have tiny (or nonexistent) benefits. The massive benefits and limited harms of social interventions are better than almost any therapy we provide in emergency medicine. People get incredibly upset about a 20 minute delay to antibiotics in sepsis, but then turn around and discharge an unhoused individual to the street with no support. (Yes, I am as guilty as you are.)
Unfortunately, despite widespread positive reporting in the media, this study is somewhat disappointing. (The general rule still applies: scientific reporting in the lay media will essentially always be wrong). This is a cluster randomized trial with 4 groups looking at unconditional cash transfers, motivational training, and coaching for unhoused individuals. Ultimately, their pre-registered outcomes looking at cognitive function and subjective wellbeing were all negative, so scientifically we should probably stop there. However, I would not have considered those to be the most important outcomes if I was designing this trial. People given the money spent 99 fewer days homeless and 55 more days in stable housing. They spent more money, but there was no difference in spending on ‘temptation goods’ such as drugs, alcohol, and cigarettes. Overall, by reducing total nights spent in shelters, the unconditional cash transfers would have actually saved society money. Of course, all of those statements are based on exploratory analyses, and so should be considered hypothesis generating only.
There are multiple limitations to this specific study. They only looked at individuals homeless for less than 2 years, with nonsevere levels of substance use, alcohol use, and mental health symptoms. They lost about half of eligible individuals to follow-up. It is a small study, and it is unclear whether $7500 is the ideal amount of money, especially in a city with as high a cost of living as Vancouver.
Bottom line: Despite being widely reported as positive in the media, this was a negative study with some interesting secondary analyses. This is a very important topic for almost every emergency department, and warrants intensive research. (If we run another RCT looking at vitamins in sepsis when we could spend that money on research like this, we should seriously question the morals of the entire medical community.)
Delayed sequence intubation
Bandyopadhyay A, Kumar P, Jafra A, Thakur H, Yaddanapudi LN, Jain K. Peri-Intubation Hypoxia After Delayed Versus Rapid Sequence Intubation in Critically Injured Patients on Arrival to Trauma Triage: A Randomized Controlled Trial. Anesth Analg. 2023 May 1;136(5):913-919. doi: 10.1213/ANE.0000000000006171. Epub 2023 Apr 14. PMID: 37058727
Delayed sequence intubation is a concept developed by Scott Weingart. I imagine everyone has heard about it, but it is basically the use of ketamine for procedural sedation with the procedure being preoxygenation. (It is a technique to allow adequate preoxygenation of agitated patients.) I believe this is the world’s first RCT of DSI. They randomized 200 adult trauma patients needing intubation to either DSI or RSI. Their primary outcome of peri-intubation hypoxia (oxygen saturation less than 93%) was significantly better with DSI (8% vs 25%, p<0.001). First pass success was higher with DSI (83% vs 69%, p=0.02) Airway related adverse events were not statistically different, but favoured DSI (9% vs 16%). There were no cardiac arrests or episodes of hypotension in this trial.
There are many problems with this study. It is small, single-centred, and unblinded. First pass success is much lower than I would expect, perhaps because it was trainees using direct laryngoscopy. They retrospectively excluded patients who had unanticipated difficult airways, but these patients might be very important in understanding the impacts of DSI. Selection bias is an issue. On the other hand, they used DSI in all comers, which should limit its efficacy (because the true benefit should be seen only in the subset who are difficult to pre-oxygenate).
Bottom line: The benefits of DSI are apparent in real time. We still need science, because there is always the potential for unanticipated harms, but it is one of the few practices that I have recommended (in the right population) without RCT level evidence. This RCT is far from definitive, but all the results point in the right direction, and make me feel comfortable leaving DSI in my tool kit for agitated patients who cannot be adequately pre-oxygenated.
DEVICE trial
The DEVICE trial: Prekker ME, Driver BE, Trent SA, et al. Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults. N Engl J Med. 2023 Aug 3;389(5):418-429. doi: 10.1056/NEJMoa2301601. Epub 2023 Jun 16. PMID: 37326325
Trying to write a brief summary of a trial comparing video and direct laryngoscopy might be dangerous. I am bound to hear some strong opinions from both sides. This is a pragmatic, open label trial comparing VL and DL in adult patients undergoing orotracheal intubation in the ED and ICU. It was stopped early, after 1420 patients, because of a benefit in the primary outcome of first pass success favouring VL (85% vs 71%, absolute risk difference 14.3% 95% CI, 9.9 to 18.7; p<0.001). However, first pass success is a surrogate outcome, and it is easily biased in an unblinded trial. All important outcomes were essentially identical between the two groups. Severe complications were identical between the two groups (21% vs 21%). Desaturation to less than 80% occurred in 10% of booth groups. Despite the headlines, this trial basically shows equivalency in all things that matter between VL and DL. (It would be difficult to show a difference, because skilled airway operators can prevent most adverse events with meticulous preoxygenation, and adequate plans to adjust course in the face of poor glottic visualisation.) There are a few other methodologic issues, which you can read about in the main blog post if you are interested.
I think the more interesting question is whether we need to continue down this line of research at all. As much as I love science, I sort of think this debate is silly. The only reason there was a debate in the past is because we were conflating two different issues. When I started, the only video laryngoscopes available were hyperangulated. Therefore, there was a significant tradeoff between the better view and impaired tube delivery. There was also a debate about whether training would adequately cross-over between the two devices. Now that standard geometry video laryngoscopes are widely available, the debate is settled. We can have the better visualisation offered by video, with no impairment of tube delivery, and perfect training. (The training is way better than before, because the standard blade can be used exactly like a direct blade, but your teacher can see exactly what is happening and so provide real time feedback.) Even the old concerns about whether you would be adequately trained in the case of an equipment failure are completely moot, because the standard geometry VL can be used as a DL. Aside perhaps for some cost questions (although almost every hospital in the countries I work in has VL already), this debate is over, and it really doesn’t need more science.
Bottom line: This large RCT demonstrated improved first pass success with video laryngoscopy, but no difference in any patient oriented outcomes. I see no reason not to use VL if it is available.
Mobile Computed Tomography at Munich Oktoberfest
Flatz W, Hinzmann D, Kampmann P, Poehlmann L, Reidler P, Schlichtiger J, Kanz KG, Ricke J, Bazarian J, Bogner-Flatz V. Mobile Computed Tomography at Munich Oktoberfest. N Engl J Med. 2023 Sep 14;389(11):1051-1052. doi: 10.1056/NEJMc2306490. PMID: 37703560
I have blasted the concept of mobile CT scans in the context of stroke, but what about in the context of a bunch of drunk idiots? (I feel OK calling them drunk idiots, because I have been one of these drunk idiots in the past.) I have worked in cities with festivals before, but nothing on the scale of Oktoberfest. Oktoberfest in Munich typically sees about 400,000 visitors per day, all attending with the explicit goal of getting hammered. You could imagine the strain that might place on local emergency departments. With the goal of reducing the number of transfers for minor head injuries, this group decided to bring a portable CT scanner (along with techs and a radiologist) to the fairgrounds in 2022, operating daily from 6pm to 2am. I will ignore the fact they decided to use a very poor decision rule (New Orleans) for assessing head injuries. They were able to perform head, c-spine, and facial bone scans. A total of 205 patients with presumed or observed mild traumatic brain injury underwent 317 scans; 191 of the cranium, 67 of the midface, and 59 of the cervical spine. Of these patients, 11 had intracranial bleeding, 23 had midface fractures, and none had cervical spine injuries. Ultimately, 17 out of the 205 patients were sent to hospital for their injuries, and another 14 because they weren’t adequately sobering up. Unfortunately, the rest of the data the present is completely meaningless when trying to assess this intervention. They talk about the number of patients “taken to local hospital and admitted for surgically treated injuries”, but that is a weird subset to focus on. The CT scanner should have no impact on the number of people requiring surgery (or, if anything, should increase that number by identifying patients that otherwise would have been missed). The only potential value would be in decreasing the total number of emergency department presentations or EMS transfers, but that number is not presented anywhere in this short research letter. Furthermore, we are given no details about the cost effectiveness of this intervention. (It might have been cheaper to just buy a standard CT scanner and a few extra beds for the local hospital, which would be more beneficial during the rest of the year.)
Bottom line: This is one of the few scenarios (giant festival of drunk trauma patients) where a mobile CT could have some utility, but unfortunately this paper does not provide any science to really let us judge the intervention.
Evidence for Anchoring Bias During Physician Decision-Making
Ly DP, Shekelle PG, Song Z. Evidence for Anchoring Bias During Physician Decision-Making. JAMA Intern Med. 2023 Aug 1;183(8):818-823. doi: 10.1001/jamainternmed.2023.2366. PMID: 37358843
This researcher is quickly becoming a favourite of mine. We previously covered a paper looking at empirical evidence of availability bias in emergency medicine. This new publication looks for real world evidence of anchoring bias. It uses a Veterans Affairs database from the United States, which means that the population is old and almost 100% male. In a sample of 108,019 adult patients with known CHF presenting to the emergency department with dyspnea, they compared testing and outcomes among those whose triage complaint mentioned CHF to those who didn’t (based on the hypothesis that a mention of CHF would bias emergency physicians towards the diagnosis of acute CHF and away from alternatives like PE.) Triage mention of CHF did decrease total PE testing (8% vs 13%) while increasing ‘CHF testing’ with BNP (81% vs 71%). (I am somewhat disturbed by how often the useless BNP is being used in clinical practice.) The key result, at least in my mind, is that despite the fact that both groups had the exact same rate of PE by 1 month (1%), many fewer of those PEs were identified in the emergency department when the triage note mentioned CHF (0.05% vs 0.24%). I also find it interesting that, even in the best case scenario, we are only identifying 1 out of 4 PEs in the ED, but that all of these numbers are below the test threshold for PE. Given what we know about PE diagnosis, that makes me think that a large number of these PEs are probably false positives. Therefore, despite successfully demonstrating anchoring bias in this data, I am not sure the authors have actually demonstrated harm (mortality is not mentioned anywhere). The major problem with this data is that it is observational and retrospective, many important factors are not recorded on the chart, and the two groups are different in many important ways that we know about. The change in testing might be a result of CHF being mentioned in the triage note, but could also be the result of some other unseen confounder. For example, the way the patient tells their story might influence both what the nurse puts in the triage note and how the doctor tests, with the triage note not influencing the doctor at all.
Bottom line: I really like this line of research. We need empirical data looking at cognitive biases, because almost all of our information about biases in medical decision making comes from case vignettes and theory. This data does seem to demonstrate the anchoring bias at work, in that the triage note influenced both testing patients received and the rate of PE diagnosis. However, the absolute differences are very small, and it isn’t clear that there is a real clinical harm here.
Family presence during cardiopulmonary resuscitation
Jabre P, Belpomme V, Azoulay E, Jet al. Family presence during cardiopulmonary resuscitation. N Engl J Med. 2013 Mar 14;368(11):1008-18. doi: 10.1056/NEJMoa1203366. PMID: 23484827 NCT01009606
This is a classic emergency medicine paper looking at family presence during cardiac arrest. They enrolled 570 family members of patients in cardiac arrest being cared for by one of 15 physician led paramedic services in France. In the intervention group, they systematically asked family members whether they wanted to be present during the resuscitation, and 79% did witness CPR. In the control group, family members were not routinely given the option to be present during CPR, and 43% witnessed CPR. The study was obviously not blinded, but the primary outcome (PTSD symptoms at 90 days) was assessed by a blinded psychologist. 27% of the intervention group had PTSD symptoms at 90 days, as compared to 37% of the control group (p=0.01; aOR 1.7 95% CI 1.2-2.5). Looking specifically at those who witnessed CPR versus those who didn’t (there was a lot of cross-over), PTSD was also lower in those who witnessed CPR. I imagine we all have experience with this by now, but they reported no significant conflicts with family members, and the time of resuscitation was the same in both groups. (Personally, I have found that family attended arrests tend to last longer, but that might be partly because of the time it takes family to arrive at hospital.) Healthcare workers reported very low levels of stress across the board, with no effect of family presence.
There are a number of potential issues that need to be considered. They don’t tell us how many people had to be screened to find these 570, and you might imagine that people who volunteer for this kind of research might be different from those who say no. They lost 17% of participants to follow-up, and the loss to follow-up was significantly higher in the control group. Because the PTSD scale used is unfamiliar, it is hard to assess the clinical significance of the numbers discussed.
Bottom line: Allowing families to be present, if they so choose, during cardiac arrest really seems to help them process the grief, with fewer psychological symptoms in the future. If, for some reason, there are still people out there a decade after this study who haven’t adopted this practice, now is the time to do it.
Irrelevant research, because you know you aren’t cleaning the ultrasound machine anyway
Peters N, Williamson F, Bauer MJ, Llewellyn S, Snelling PJ, Marsh N, Harris PNA, Stewart AG, Rickard CM. Comparison of Low-Level to High-Level Disinfection in Eliminating Microorganisms From Ultrasound Transducers Used on Skin: A Noninferiority Randomized Controlled Trial. J Ultrasound Med. 2023 Jun 12. doi: 10.1002/jum.16286. Epub ahead of print. PMID: 37306253
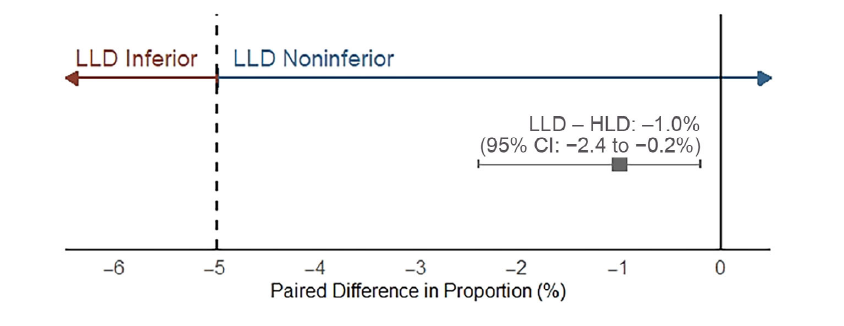
This is a relatively simple study comparing two types of disinfectant for sterilisation of ultrasound probes. I don’t know either of these brands (Tristel vs Clinell), but high-level disinfection is apparently defined as disinfection that removes more resistant species, such as mycobacterium and C difficile spores. For such a simple study, they have a ridiculously huge sample size, with 654 participants. Partly, this is because they only included people who had bacteria cultured from both forearms, so we end up with 478 people being analysed.
High level disinfection led to complete sterility in 99.6% of cases, and low level in 99.0% (95% CI: 97.6–99.7%), which fell within their predefined non-inferiority margin of 5%. Interestingly, they appear to demonstrate a statistical difference between the two groups, demonstrating that the low level is actually inferior, just not inferior at the level that they predefined, which is why non-inferiority trials are a mess. However, considering we are talking about a surrogate outcome, rather than clinical infections, and they are close to identical, I imagine the authors are correct in their claim of ‘non-inferiority’ when it comes to real world practice. Apparently the low level wipes are much easier to use, but I haven’t used either, so I don’t really get the difference.
A few points:
- This study makes me wonder whether we really understand the purpose of randomization in medicine. Did we really think there was going to be a difference between the left and right forearm that could systematically skew this data? Even if one arm was dirtier, the outcome was the proportion of bacteria removed during disinfection, with both measurements occurring after the probe touched the arm. Did randomising here add anything of value at all?
- The requirement for 60 seconds of drying after disinfection makes me wonder about clinical applicability. Obviously, this is fine if people are cleaning up after themselves, but I find this is rarely the case. Therefore, I am required to clean the probe just before starting a procedure. Have you ever met an emergency physician with the patience to wait a full 60 seconds just for sterilisation to occur before starting a procedure?
- If the value of high-level disinfection lies in removing rare bacteria, such as mycobacteria or C diff, does it make sense to test this in low risk volunteers? More importantly, as much as I love the mediaeval sound of horse-blood agar, we know that mycobacteria are very hard to culture, so perhaps standard plating techniques won’t demonstrate the value of the higher level disinfectants?
- I am not sure the surrogate outcome of colony forming units matters all that much. Bacteria are everywhere in the world. Is perfect sterility really needed for minor procedures, such as IV starts? (After all, we don’t use sterile gloves for IV starts.)
Bottom line: As long as my colleagues clean the ultrasound machine after use, I honestly don’t care what they use. Seriously. Just clean the bloody thing.
More irrelevant research, because we don’t stock platelets at either of my hospitals
van Baarle FLF, van de Weerdt EK, van der Velden WJFM, et al. Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia. N Engl J Med. 2023 May 25;388(21):1956-1965. doi: 10.1056/NEJMoa2214322. PMID: 37224197
This is an RCT looking at patients with thrombocytopenia (between 10 and 50,000 platelets per mm3) who needed central lines placed, and randomizing them to 1 unit of prophylactic platelet transfusion or no transfusion. They designed it as a non-inferiority trial, but ultimately transfusion resulted in significantly less bleeding (4.8% of the transfusion group and 11.9% of the no-transfusion group, (ARR 7.1%, 90% CI 1.3-17.8%). Unfortunately, this is an unblinded trial, which is problematic both because the bleeding scale used is somewhat subjective, but also because the physicians knew the purpose of the trial and might have approached these procedures differently than usual. The big issue in applying these results is that many community hospitals don’t stock platelets, including both hospitals I work at, which means you still need to make a judgement call about the urgency of the central line versus the small but seemingly real increase in bleeding seen here.
Bottom line: I will attempt to transfuse platelets prior to CVC placement in patients with platelet counts below 50,000, but realistically that means deciding whether the patient is healthy enough to wait until they are in the ICU before having their line placed.
Busting myths I didn’t even know existed
Sun YI, Oliver JD. Hot Sauce: No Elimination of Vibrio vulnificus in Oysters. J Food Prot. 1995 Apr;58(4):441-442. doi: 10.4315/0362-028X-58.4.441. PMID: 31137341
I work very very hard to find you the cream of the crop of the medical literature. This time, we are going back 30 years to the Journal of Food Protection, for some highly pertinent and probably cutting edge information about oysters and everyone’s favourite little microbe, Vibrio vulnificus. Given that V Vulnificus apparently causes 95% of seafood borne deaths in the United States, researchers were previously very excited to announce that Tabasco sauce kills the bacteria in a petri dish. This is a follow up study, in which oysters were artificially exposed to V Vulnificus and then either coated with Tabasco sauce, horseradish, or nothing for 10 minutes before being tested for V Vulnificus and total bacterial levels. I was actually somewhat shocked that Tabasco completely eliminated V Vulnificus from the surface of the oysters (while horseradish did nothing). However, don’t get too excited, because there was an order of magnitude more bacteria inside the oysters than on their surface, and Tabasco had absolutely no effect on that population.
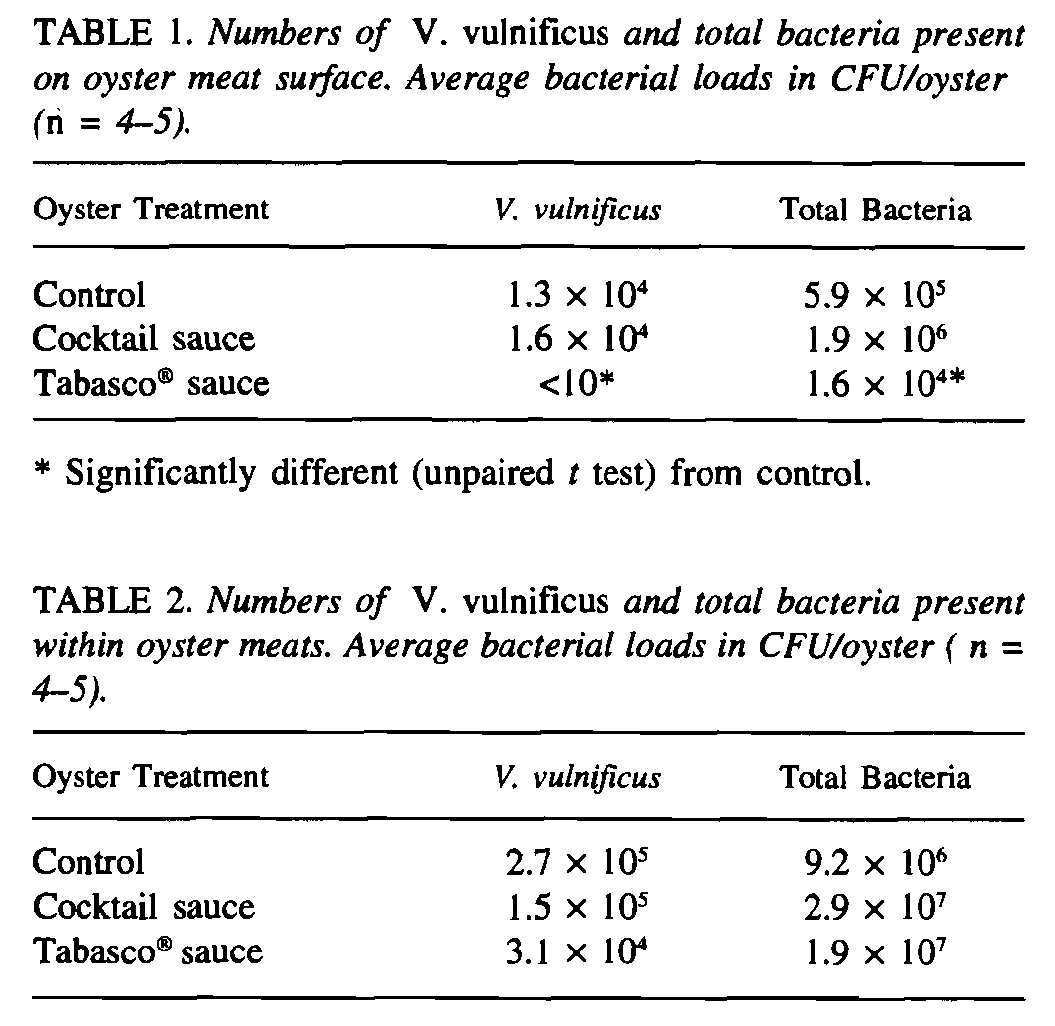
Bottom line: Although Tabsco probably won’t save you from a painful death at the hands of V Vulnificus it does seem to have inherent antibacterial properties, so maybe do a few shots next time you feel pharyngitis coming on?
Cheesy Joke of the Month
I recently invented a mind controlled air freshener
It makes scents if you think about it



One thought on “Research Roundup (Perth live edition)”
Re Dwyer et al paper, may I remind you that poverty is a crime, not a profitable disease! (sarcasm intended).