
Morgenstern, J. The Research Roundup (February 2024), First10EM, February 26, 2024. Available at:
https://doi.org/10.51684/FIRS.134525
Welcome back to another edition of the research roundup, where we discuss an eclectic collection of articles selected through the very rigorous process of whatever I happened to find interesting in my recent reading. The BroomeDocs podcast version can be found here: https://broomedocs.com/category/podcast/
Putting nail bed repair to bed?
Jain A, Greig AVH, Jones A, Cooper C, Davies L, Greshon A, Fletcher H, Sierakowski A, Dritsaki M, Nguyen TTA, Png ME, Stokes JR, Dakin H, Cook JA, Beard DJ, Gardiner MD; NINJA Collaborative. Effectiveness of nail bed repair in children with or without replacing the fingernail: NINJA multicentre randomized clinical trial. Br J Surg. 2023 Mar 30;110(4):432-438. doi: 10.1093/bjs/znad031. PMID: 36946338
This is a multicenter pragmatic trial from 20 hand surgery units in the United Kingdom that looked at whether there was any value in replacing the finger nail (or a foil surrogate if the nail was not available) after nail bed laceration repair in children. They enrolled 451 children, and all of their results were completely negative, with a possible hint of more infections when you put the nail back on. How well these results extrapolate to emergency practice or adults is an open question, but this is by far the best data we have, and it is pretty clear we shouldn’t be wasting time putting the finger nail back in place. However, this study doesn’t address the bigger issue: is there any value in suturing the nail bed at all? There are previous studies that suggest no, and physiologically, a fingernail that is in place is probably going to do a much better job splinting the wound in the correct position than sutures ever could. Personally, I never remove fingernails to examine the growth plate, which means that despite being very well done, this study is mostly pointless. (This group says that they are planning on running another study asking the bigger question of whether nail bed laceration repair is required at all, so hopefully we will return to this topic again in the future.) I will also point out that there is good evidence that dermabond is just as effective as sutures for nail bed repair, so if the nail is already completely removed, that is my go to.
You can read the full write up for this paper here.
Bottom line: This is a well done RCT that demonstrates pretty convincingly that you should not bother trying to put fingernails back on after nail bed repair (and my guess is you definitely shouldn’t be removing them either).
MINTing a new transfusion strategy?
Carson JL, Brooks MM, Hébert PC, et al; MINT Investigators. Restrictive or Liberal Transfusion Strategy in Myocardial Infarction and Anemia. N Engl J Med. 2023 Nov 11. doi: 10.1056/NEJMoa2307983. PMID: 37952133
This is a big multicenter RCT comparing liberal and restrictive transfusion targets in patients with MI. (They essentially used the normal targets of 70 g/L and 100 g/L, but with more leeway in the 70-80 g/L range.) They included 3504 patients, and their composite primary outcome of MI and death was not statistically significant, but in a way as will create a lot of debate. (The 95% confidence interval either exactly touches 1, or goes to 0.99, depending on which calculation you use.) In absolute terms, 16.9% of the restrictive group had death or MI as compared to 14.5% of the liberal group. This difference seems to be split evenly between death and MI, which is good because the nonfatal MIs are likely meaningless. When almost all of the 95% confidence interval suggests benefit from the liberal group, it seems fair to conclude that liberal transfusion is better, but that would overlook the effect of bias in research, and the fact that we use very lax statistical cutoffs in medical research. This was an open label trial, which introduces a significant risk of bias, and therefore I think you need to downgrade your confidence in the results significantly. Furthermore, there is evidence of harm in the liberal group, with significantly more patients having to drop out of the trial due to adverse events. This is all complicated by the fact that they included patients with both type 1 and type 2 MIs, when one might guess that demand ischemia requires a different approach. The only real answer here is ‘we don’t know’. Personally, I think this suggests that baseline care should probably be closer to the restrictive group, in an effort to limit harms, but with significant leeway for more liberal transfusion based on clinical judgment. However, if you want to argue the opposite (that your baseline is going to be liberal but with significant leeway for a more restrictive approach based on judgment and patient preference), I couldn’t really argue against that.

Bottom line: This is our biggest trial looking at liberal versus restrictive transfusion in the context of MI, and we are left without a clear answer.
Routine MRI for first episode psychosis?
Blackman G, Neri G, Al-Doori O, Teixeira-Dias M, Mazumder A, Pollak TA, Hird EJ, Koutsouleris N, Bell V, Kempton MJ, McGuire P. Prevalence of Neuroradiological Abnormalities in First-Episode Psychosis: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2023 Oct 1;80(10):1047-1054. PMID: 37436735
Based on scientific quality, this is the type of paper I usually ignore. However, based on previous demands for ‘medical clearance’ by psychiatry teams, I fear that someone might try to use this paper to obstruct admissions from the ED, so I wanted to briefly point out its flaws. It is a systematic review and meta-analysis looking at MRI brain findings in patients with first episode psychosis. The headline finding was that the overall prevalence of MRI abnormalities was 26%, and 6% of these were considered to be ‘clinically relevant’. Based on those numbers, the authors conclude “it is becoming increasingly difficult to justify not making MRI a mandatory part of the clinical assessment of [first episode psychosis]”, and I am worried that conclusion could be used to delay appropriate psychiatric referrals. However, when you dig deeper, I actually think this data might be a stronger argument against routine MRI than for it. Although 10 of the 12 papers specifically excluded patients in whom a secondary cause of psychosis was suspected, these are not consecutive data sets, and selection bias is likely to be a huge issue. (We don’t order MRIs on all patients with first episode psychosis. In order to get an MRI, these patients are all special in some way. These authors don’t have access to individual patient data, so can’t even guess what made these patients special.) More importantly, we know that MRI finds a ton of things that have absolutely no clinical utility, and when you dig through their supplementary data, it seems pretty clear that almost all these findings are incidental. The MRIs were generally ordered to “rule out brain mass”, and the prevalence of tumors was only 0.1%. The MRI abnormalities were things like “white matter changes” and “atrophy”. What about the finding that 6% were “clinically relevant”? Well, their definition of clinically relevant was “any referral based on the findings”, so if the psychiatrist sent the patient to a neurologist and got a note back saying “don’t worry, that MRI finding is completely meaningless (also, please stop ordering pointless MRIs and sending all the patients for pointless neurology consults afterwards)” that consult would have been considered ‘clinically relevant’. Perhaps most importantly, these MRIs were performed an average of 1-2 years after the initial onset of psychosis. In other words, there is absolutely no urgency, and these studies should never delay psychiatric consults in the ED. If, based on specific findings on history or physical, MRI is thought to be warranted, it can be arranged as an outpatient by the psychiatrist or primary care physician.
Bottom line: Patients with first episode psychosis do not need routine MRIs based on this data. They do need a careful history and physical, as a subset will have pathology. MRIs may be warranted in a small subset of patients, but those MRIs do not need to occur in an emergency department.
Should we (psych) stop downplaying substance induced psychosis?
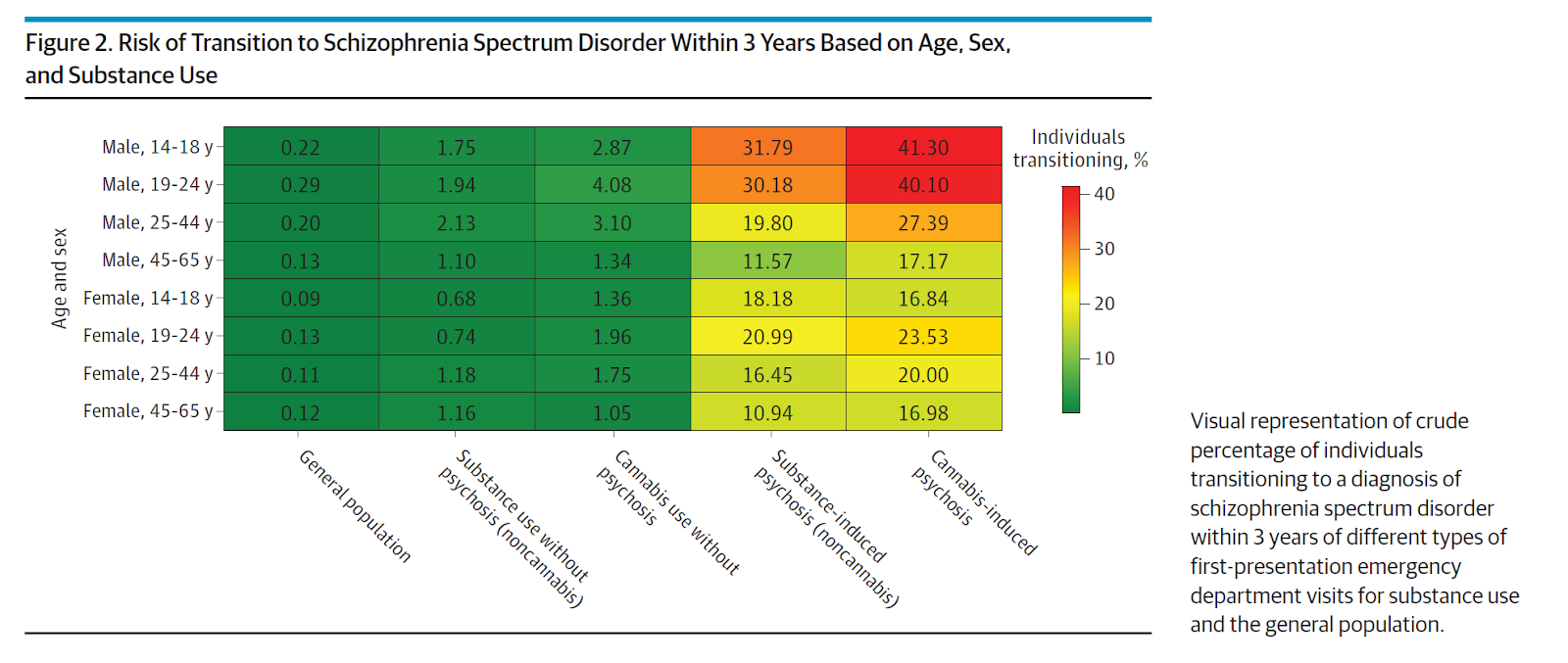
Myran DT, Harrison LD, Pugliese M, Solmi M, Anderson KK, Fiedorowicz JG, Perlman CM, Webber C, Finkelstein Y, Tanuseputro P. Transition to Schizophrenia Spectrum Disorder Following Emergency Department Visits Due to Substance Use With and Without Psychosis. JAMA Psychiatry. 2023 Sep 27:e233582. doi: 10.1001/jamapsychiatry.2023.3582. PMID: 37755727
I think this paper is interesting, and potentially important. I frequently get push back from psychiatry about referrals for drug induced psychosis. Their argument seems to be to “just tell the patient to stop taking drugs and their psychosis will resolve.” That argument has always seemed ridiculous to me, as we know most drug use is chronic, and therefore drug induced psychosis is also likely to be chronic and recurrent, requiring ongoing psychiatric care. However, it seems like the issue is even bigger than that, because substance induced psychosis is associated with a significantly increased risk of a future diagnosis of schizophrenia. This is a massive database trial from Ontario. They focused on patients without a history of psychosis (no visits for psychosis in the prior 2 years). They identified a cohort of patients presenting to the ED with substance use (407,373 over the 14 years) and then a subset with substance induced psychosis (13,784 patients). In the following 3 years, 19% of the patients with substance induced psychosis had transitioned to a formal diagnosis of schizophrenia. (Of course, this means that 80% didn’t transition. I imagine psychiatry might emphasize that number, but a 20% long term risk combined with current active psychosis seems high enough to warrant psychiatric care in my mind.) The rate varied by drug type, with 9% of alcohol and 26% of cannabis patients transitioning). For comparison, patients in the ED with substance abuse but no psychosis had a 3% rate of transitioning to a diagnosis of psychosis. As compared to the general population, patients with substance induced psychosis have a 163 fold increased rate of being diagnosed with schizophrenia within 3 years.
Bottom line: Substance abuse and psychiatric disease go hand in hand. Doctors who treat one must be experts in the other as well. We do not do our patients any favours by deflecting their care.
Consequences of a Health System Not Knowing Which Patients Are Deceased
Wenger NS, Sanz Vidorreta FJ, Dudley MT, Walling AM, Hogarth M. Consequences of a Health System Not Knowing Which Patients Are Deceased. JAMA Intern Med. 2023 Dec 4:e236428. doi: 10.1001/jamainternmed.2023.6428. Epub ahead of print. PMID: 38048124
This is a primary care research letter, so seemingly not that important to emergency medicine. However, we often discuss research conducted on databases, and we are going to see a huge increase in the number of AIs trained on EHR databases, so I think it is important to remind ourselves how inaccurate EHRs are. This research focused on primary care patients known to be seriously ill. They looked at 11,698 patients, and over the 2 year study period 3596 died. However, 676 (20%) of these patients were still marked as alive in the primary care EHR system. They talk about some primary care issues, like the number of phone calls and messages sent to these patients despite the fact they were dead, but I just wanted to include this to remind people to be very wary of studies using data from EHRs, and to be especially wary of the accuracy of early generations of AI in medicine.
ACEP backs topical anesthetics for simple corneal abrasions
Green SM, Tomaszewski C, Valente JH, Lo B, Milne K. Use of Topical Anesthetics in the Management of Patients With Simple Corneal Abrasions: Consensus Guidelines from the American College of Emergency Physicians. Ann Emerg Med. 2024 Feb 6:S0196-0644(24)00004-0. doi: 10.1016/j.annemergmed.2024.01.004. PMID: 38323950
This is not really news, as we have covered the evidence ad nauseum in the past, but I know some people are still more comfortable with changing practice when there are official guidelines. After a systematic review of the evidence, and a guideline process which you can read more about in the main post, ACEP tells us that “in adult ED patients with simple corneal abrasions as defined in these guidelines, it appears safe to prescribe or otherwise provide a commercial topical anesthetic (ie, proparacaine, tetracaine, oxybuprocaine) for use up to every 30 minutes as needed during the first 24 hours after presentation as long as no more than 1.5 to 2 mL total (an expected 24-hour supply) is dispensed and any remainder is discarded after 24 hours.”
Bottom line: A shared decision making conversation is still a good idea (if only to prepare patients for a future ophthalmology tirade), but I have yet to have a patient decline short term use of topical anesthetics to control the pain from their corneal abrasion.
Have we been overly optimistic about REBOA?
Jansen JO, Hudson J, Cochran C, et al. Emergency Department Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial. JAMA. 2023 Oct 12. doi: 10.1001/jama.2023.20850. PMID: 37824132
This is the first RCT of REBOA in trauma, and it had to be stopped early after 90 patients were enrolled because of increased mortality in the REBOA group (54% vs 42%, OR 1.58, 95%CrI 0.72-3.52). Based on their Bayesian analysis, they conclude a 87% chance that REBOA increases mortality and only a 4% chance that it decreases mortality. As discussed in the main post, procedural studies can be difficult to interpret, because not only does the procedure need to be effective, but the operators also need to be skilled. I have never used REBOA, but it is possible that operator skill was an issue in this trial, given that they failed to even cannulate the artery 17% of the time. The REBOA was only used in half of the REBOA group, and it is very hard to show benefit from a device you didn’t actually deploy. Furthermore, because of the ‘stay and play’ paramedic services in the UK, these patients were arriving to the trauma center an average of 90 minutes after their injury, so they might have just been deploying REBOA too late to make a difference. Therefore, there are many reasons that research should continue in this area, but no reason to be using REBOA clinically outside of those research studies.
Bottom line: In our only RCT of REBOA in trauma to date, REBOA increased mortality, and therefore the device is clearly not ready for clinical use.
Most people “knew” this already, but this is my favorite paper of the month
Siebert JN, Salomon C, Taddeo I, Gervaix A, Combescure C, Lacroix L. Outdoor Cold Air Versus Room Temperature Exposure for Croup Symptoms: A Randomized Controlled Trial. Pediatrics. 2023 Sep 1;152(3):e2023061365. doi: 10.1542/peds.2023-061365. PMID: 37525974
I love this study, because it uses an RCT to answer a simple question that I think most people would have said couldn’t be addressed with an RCT. They took 118 children with moderate croup, and randomized them to either stay outside in the cold air (when temperatures were less than 10 degrees Celsius) or to wait inside. At 30 minutes, more kids in the cold air group had improvement of their croup symptoms, defined as 2 or more points better on the Westley Croup score (49% vs 24%, OR 3.1, 95% CI 1.4-6.8, p=0.007) However, this difference was gone by 60 minutes, as both groups continued to improve. This is far from a perfect study. It is an unblinded study with a very subjective outcome, so there is a very high risk of bias and you should have low confidence in their results. Furthermore, although they don’t report any adverse events, it doesn’t sound like they checked temperatures after this exposure, and the outdoor temperatures here were almost always between 0 and 10 degrees, so be careful extrapolating these results to frigid Canadian winters. That being said, this is the best evidence we have, and there does seem to be a short term symptom benefit.
Bottom line: This is by far the best evidence we have on the topic, and perhaps the best evidence we will ever see. If you are looking for short term symptom relief, and you are careful about avoiding harms, it seems reasonable to counsel parents about using cold air to improve symptoms from croup.
Speaking of breathing, a rebuke to breathwork?
Fincham GW, Strauss C, Cavanagh K. Effect of coherent breathing on mental health and wellbeing: a randomised placebo-controlled trial. Sci Rep. 2023 Dec 13;13(1):22141. doi: 10.1038/s41598-023-49279-8. PMID: 38092805
Breathing exercises of all sorts have been popularized as an important part of health. I have listened to FOAMed heroes talk about breathwork. I have participated in breathwork sessions at conferences. I have discussed the importance of breathing in performance under pressure. Is it possible, like much ‘health’ dogma, that this is all bunk? This is a very well done RCT of the practice, with an intervention group using guided breathing at rate of 5.5 breaths a minute (usual slow breathing as recommended by practitioners of breathwork), and a control group using the exact same guided breathing audio, but at a rate of 12 breaths a minute (the low end of normal, and a rate not suggested by breathwork practitioners). Participants were supposed to do a 10 minute guided breathing session every day for 28 days. They enrolled 394 participants, and had them perform surveys on stress, anxiety, sleep, and overall well being on day 1, day 28, and then 4 weeks after the intervention. There is no need to get into the numbers, as they were identical between the two groups across every single data point. That being said, numbers were improved from baseline in the 12 breaths a minute group, so it is possible that the specific pattern of breathing is irrelevant, and just spending 10 quiet minutes breathing every day is all that matters. Of course, there are many other limitations to a study run online and using self-assessment surveys, so the results are far from definitive. The biggest issue is probably that this is looking at long-term, preventative outcomes, whereas when breathing is taught in emergency medicine and critical care circles, we are talking in the moment, acute stress reduction. It isn’t clear that you need the same large RCT to see that breathing exercises works in the moment. (When I can get my toddler to breathe, the tantrums seem to settle.) All that being said, much like the croup paper, I think these authors deserve a lot of credit for running a well designed, controlled RCT of a practice that usually doesn’t get rigorous research.
Bottom line: This is the highest quality study of breathwork to date, and it is pretty definitively negative. I think this tells us that specific breathing patterns are unlikely to be helpful for long term overall well being, but still leaves open the possibility that a daily practice of quiet breathing (at any rate) could have beneficial effects. Furthermore, this research doesn’t comment on potential short term benefits when breathing is used reactively in moments of stress..
Esophageal food boluses need endoscopy, not medical management
Tiebie EG, Baerends EP, Boeije T, Frankenmolen PG, Lameijer H, van den Berg W, van Stralen KJ, Ridderikhof ML, Bredenoord AJ. Efficacy of cola ingestion for oesophageal food bolus impaction: open label, multicentre, randomised controlled trial. BMJ. 2023 Dec 11;383:e077294. doi: 10.1136/bmj-2023-077294. PMID: 38081653
We have covered ‘medical management’ of esophageal food bolus a number of times before (eg, here and here). The bottom line is that, although the on-call doctor often requests this as a delay tactic, this is an anatomical problem that requires endoscopy, not medical management. One popular trick that I have not covered from an EBM stand point is the use of carbonated beverages. This is an open label, multicentre, randomized controlled trial from the BMJ Christmas edition comparing cola ingestion to nothing in 51 adult patients presenting with spontaneous esophageal food bolus impaction. The cola group was given 25 mL cups of cola, repeated up to 8 times (200 mL total). The cups were given 1 min apart, with a 10 minute pause between cup 4 and 5. As you might expect, despite the widespread use of this technique, there was absolutely no difference. Improvement occurred in 61% of both groups. Time to complete passage was the same (40 vs 45 minutes). Endoscopy rates were the same. (Of note, European guidelines suggest endoscopy within 6 hours if no resolution, which is unattainable at any institution I have ever worked at.) There were no serious adverse events, but 21% of the cola group reported an increase in pain after drinking cola. A key finding of this paper, as well as the many other papers looking at medical management of esophageal food boluses, is that many will resolve spontaneously. If GI wants to monitor the patient prior to endoscopy, that is fine. However, medical management is net harmful, and so should not be included in the waiting period.
Bottom line: Cola ingestion changes nothing, but does increase pain, and therefore should be avoided.

The 10 commandments of emergency medicine
Evans CS, Slovis C. Revisiting the Ten Commandments of Emergency Medicine: A Resident’s Perspective. Ann Emerg Med. 2021 Mar;77(3):367-370. doi: 10.1016/j.annemergmed.2020.10.013. PMID: 33618812
30 years ago, Corey Slovis published a paper entitled “The Ten commandments of Emergency Medicine”. This paper revists those commandments 30 years later to discuss what might have changed. Not science, but it is an interesting paper that might provoke some discussion or thought. The 10 few commandments (with their original for comparison) are:
- Secure the ABCs, but carefully [vs “secure the ABCs”]
- Remember naloxone, glucose, and thiamine [vs “consider or give naloxone, glucose, and thiamine”]
- Administer a pregnancy test (and sometimes a bedside ultrasound) [vs “administer a pregnancy test”]
- Assume the worst [vs assume the worst]
- Do not send unstable patients to radiology, but if you must, do no send them alone [vs “Do not send unstable patients to radiology”]
- Seek out the red flags [vs “Look out for the common red flags”]
- Trust no one, believe nothing (not even the electronic health record [vs “Trust no one, believe nothing (not even yourself)]
- Learn from your mistakes [vs “Learn from your mistakes”]
- Do unto others as you would your family (and that included families different from yours) [vs “Do unto other as you would your family (and that includes coworkers)”]
- When in doubt, always err on the side of the patient [vs “When in doubt, always err on the side of the patient”]
Most of these changes are relatively obvious, and reflect clear changes in emergency medicine. We are a little more cautious in resuscitation, recognizing that jumping straight to things like airway management can cause harm. We like ultrasound. There are more caveats, which may simply represent a physician with a few extra decades of wisdom, realizing that things are rarely black and white, even when you are trying to write the ten commandments. For the most part, I think these are reasonable axioms for emergency physicians to live by, although I think there are major problems with “assume the worst”. I think this commandment, and the broader mentality, has probably done tremendous harm. I imagine things were different when Corey first wrote this back in 1990, but this assumption has led to massive overtesting, false positives, and overdiagnosis in emergency medicine. I think “consider the worst” might be a reasonable approach. Considering the worst doesn’t imply that every condition must be tested for, only thought about. (Although even that can bias our thinking.) But “assume the worst” is a mentality that I think causes tremendous harm to this day.
Cheesy joke of the month
I got to the restaurant a little early for my reservation, and the manager asked if I was OK waiting for a bit.
Of course, I told him that was fine.
He said, “Great!. Take these drinks to table 9.”


2 thoughts on “The Research Roundup (February 2024)”
“That being said, numbers were improved from baseline in the 12 breaths a minute group, so it is possible that the specific pattern of breathing is irrelevant, and just spending 10 quiet minutes breathing every day is all that matters.” Isn’t that in fact the most likely conclusion?
Its hard to separate that from simple regression to the mean. People volunteering to participate in a study like this might be expected to be in a somewhat more stressful state of life than the average, and simply allowing time to pass might bring the average person make to a normal state. In fact, as compared to 10 minutes of breathing, I think that bias is probably the more likely explanation, but both are possible.