ECG Blog #427 — To Cath this Elderly Patient?
Ken Grauer, MD
APRIL 26, 2024
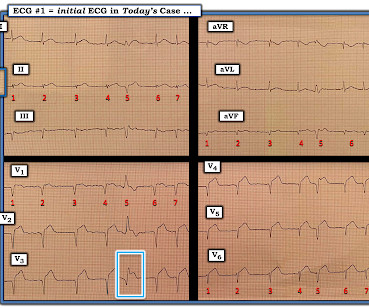
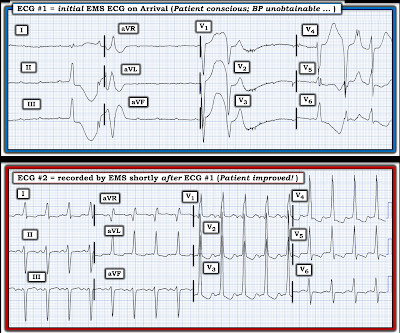
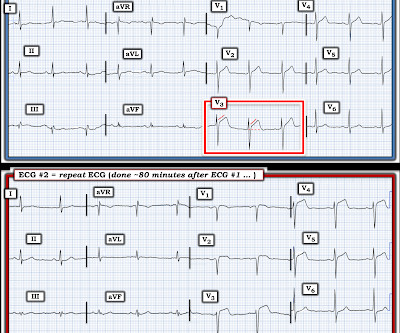
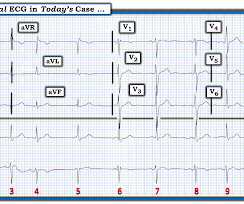
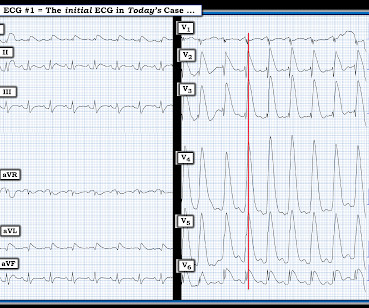
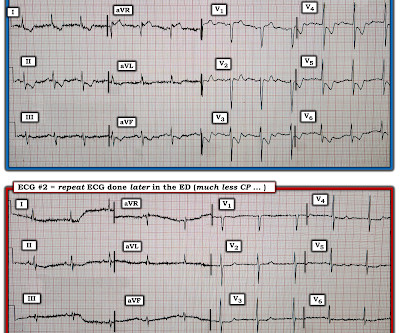
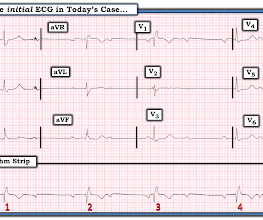
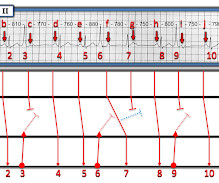
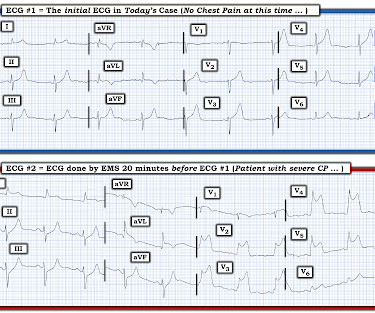
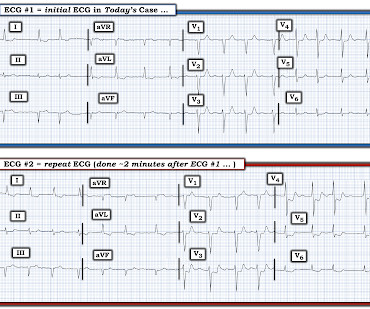
The ECG in Figure-1 — was obtained on the scene by EMS ( E mergency M edical S ervices ). The patient was a man in his 90s, who ~1 hour earlier, noted the onset of severe CP ( C hest P ain ). He was hemodynamically stable — but clearly distressed with a sense of “impending doom” at the time ECG #1 was recorded. Despite the patient’s age — he was independent, lived alone, had good mental function — and had family support.






Let's personalize your content