

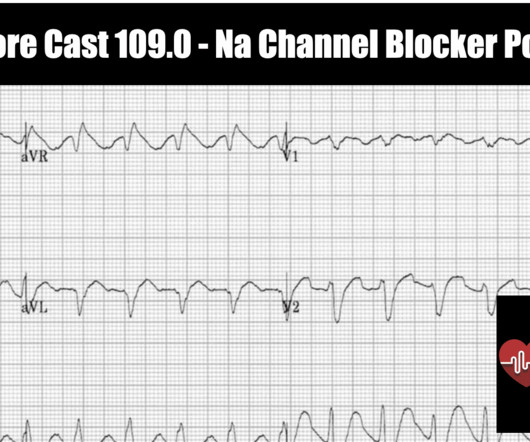
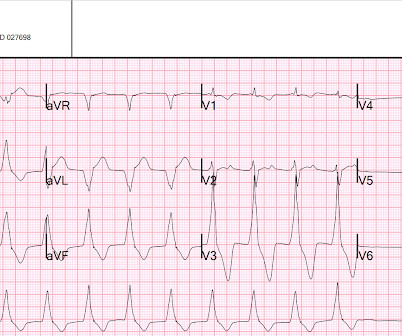
REBEL Core Cast 109.0 – Na Channel Blocker Poisoning
RebelEM
SEPTEMBER 27, 2023
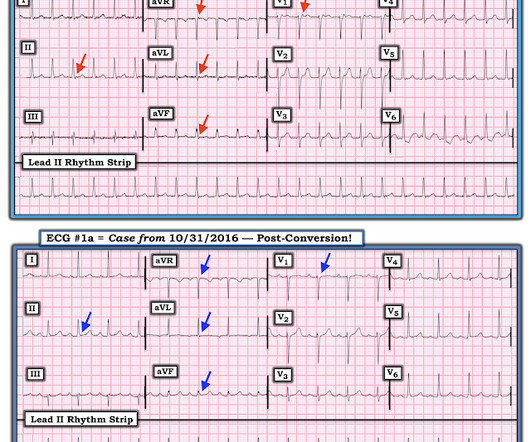
A newly “wide QRS”, especially with hemodynamic instability, should prompt consideration of sodium channel blockade and not ventricular tachycardia. Authors evaluated the relationship between QRS duration and negative clinical events in patients with confirmed tricyclic anti-depressant (TCA) poisoning. Boehnert 1985 ). Read more








Let's personalize your content