

ECG Blog #430 — Just a Regular LBBB ECG?
Ken Grauer, MD
MAY 16, 2024
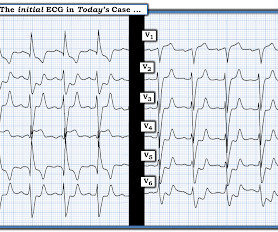
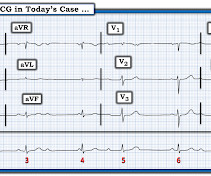
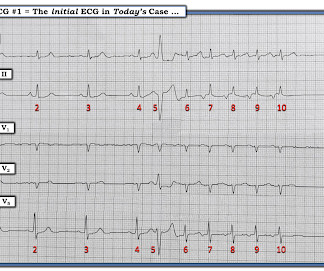
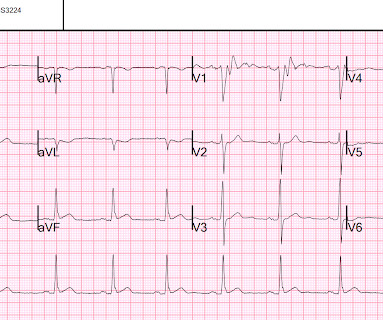
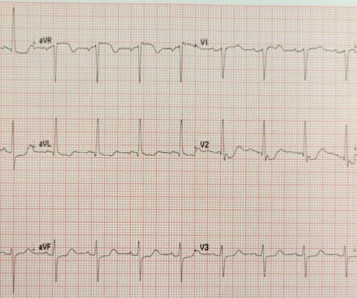
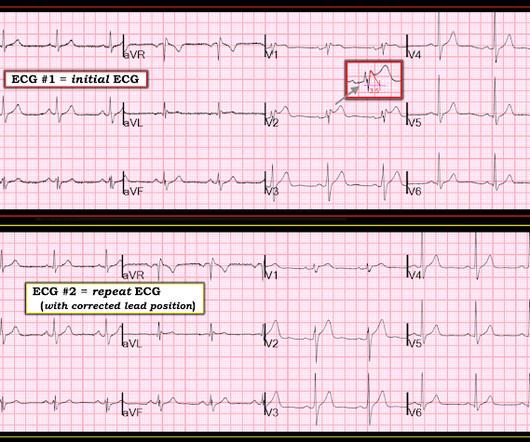
The ECG in Figure-1 — was obtained from an older man who had just completed dialysis — and , is now complaining of abdominal discomfort that radiates to his chest. Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). How would YOU approach this case?















Let's personalize your content