

emDOCs Videocast: EBM Update – Fluids in Pancreatitis and Hypertriglyceridemic Pancreatitis
EMDocs
FEBRUARY 20, 2024
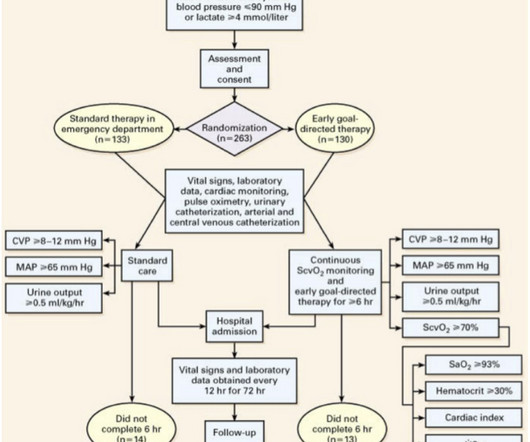
Fluids in Pancreatitis #1 : de-Madaria E, Buxbaum JL, Maisonneuve P, et al; ERICA Consortium. Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis. cc/kg/hour of LR Control: LR Bolus of 20 cc/kg (regardless of fluid status) followed by 3.0 2.18) Fluid Overload: 20.5% 2.18) Fluid Overload: 20.5%

























Let's personalize your content